
Adrenal Washout Calculator (CT)
?Bookmark this page for future reference (‘Ctrl+D’ (Windows)/ ‘⌘ +D’ (Mac users).
Table of contents:
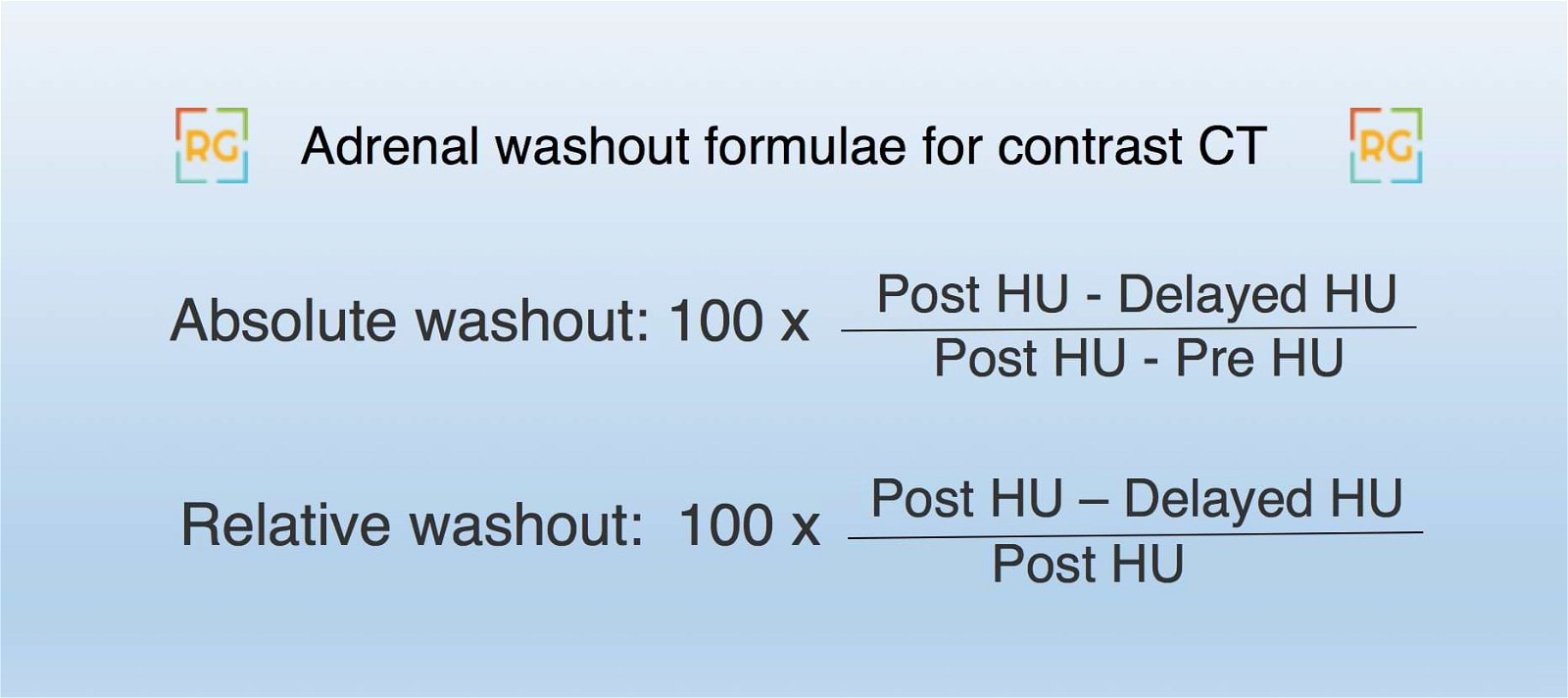
CT Adrenal wash out formulae:
How to measure attenuation of adrenal adenomas on CT?
ROIs (Region of Interest) should be placed within the nodule encompassing two-thirds of its circumference to obtain a measurement that is as accurate and representative as possible.

What is Adrenal Mass Protocol CT?
Adrenal protocol CT is performed for characterizing incidentally detected adrenal lesions (incidentalomas). It consists of :
- A non-contrast CT -> If the adrenal lesion characteristics are that of a benign lesion (adenoma/myelolipoma), no further imaging is necessary.
- Post-contrast CT at 70 secs delay.
- Delayed CT at 15 minutes.
To avoid excess radiation dose to the patient (ImageWisely), the CT can be tailored to cover only the adrenal glands.
Tips and tricks for Adrenal lesion characterization:
- An incidental adrenal mass that is <1 cm in the short axis need not be pursued.
- Attenuation value of less than 10 HU on unenhanced CT is diagnostic of an adrenal adenoma. This is owing to intra-cytoplasmic fat. Note that MACROSCOPIC fat suggests and adrenal myelolipoma and not an adenoma (Refer to spotter case 6 from case set 11).
- Unenhanced HU of more than 43 HU in a noncalcified, non-hemorrhagic lesion is suspicious for malignancy, regardless of washout characteristics.
- One-third of adenomas are lipid-poor. These can be diagnosed using
- Chemical shift MR imaging (CSI) – Drop of signal on out of phase MRI sequence (Spotter case 1 in the case set number 17).
- If the unhenanced HU value is more than 20, multiphase contrast CT is preferred over CSI MRI imaging. This includes an unenhanced scan and post-contrast images at 70 seconds and 15-min. Adenomas washout early while other lesions don’t. Absolute percentage washout (APW) more than 60% and relative percentage washout (RPW) more than 40 % suggests an adenoma. Refer to the formulae for calculating adrenal washout.
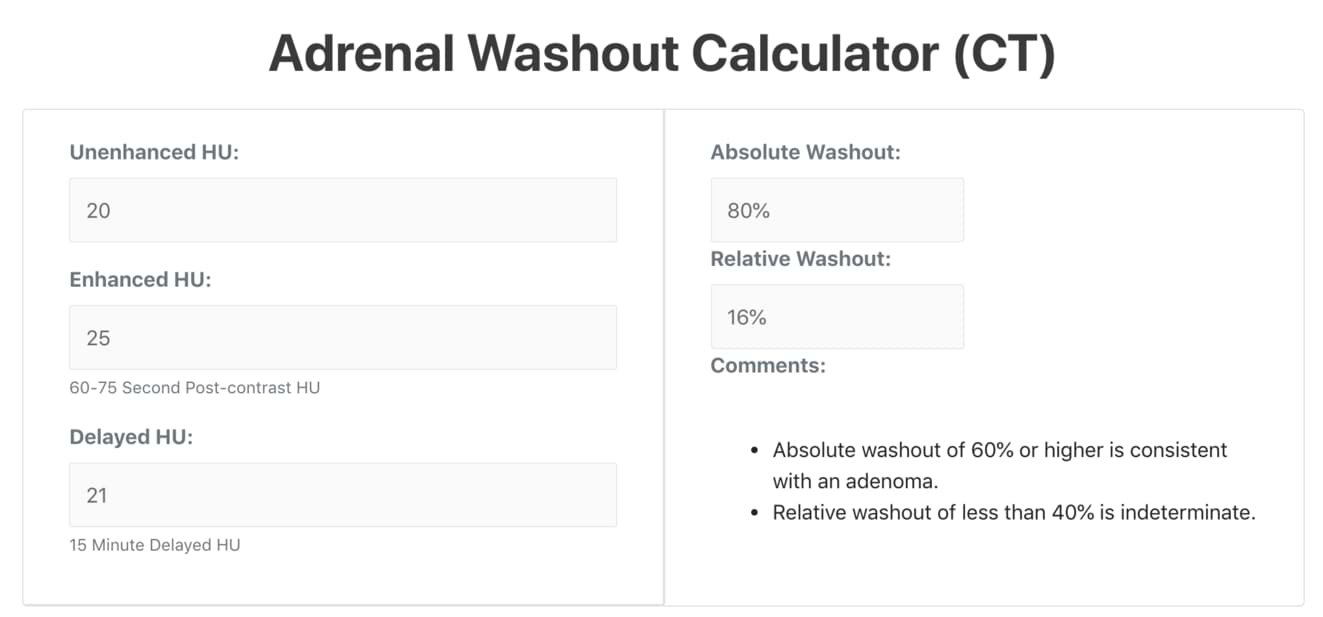
- Use the adrenal washout calculator to calculate APW and RPW for indeterminate adrenal lesions.
-
-
- False-positive values for APW and RPW include:
- Adrenal metastases from hypervascular lesions like hepatocellular carcinoma and renal cell carcinomas: Compare with prior imaging studies and/or biopsy.
- Pheochromocytomas: These enhance>100 HU on arterial phase & >130 HU on the venous phase while an adenoma does not enhance this much.
- False-positive values for APW and RPW include:
- Benign adrenal masses include:
- Lipid-rich adenoma
- Myelolipoma
- Cyst
- Hemorrhage, in the appropriate clinical setting.
- Lesions with benign calcifications
- Lesions which are indeterminate can be further characterized:
- Size: Size less than 4 cm and interval stability of more than a year favors benign etiology.
- Known malignancy raises the risk of malignant lesions.
- Peripheral enhancement should raise concern for metastasis in the setting of primary malignancy
- In suspicious cases, an image-guided biopsy is the next best step.
-
What is an adrenal incidentaloma?
An adrenal incidentaloma is an adrenal mass measuring greater than 1 cm that is discovered during a radiologic examination that was performed for indications other than evaluation of adrenal disease.
Differentiating adrenal myelolipoma vs adenoma on CT:
Adrenal myelolipoma has MACROSCOPIC fat while adenoma has microscopic fat.
- Myelolipomas are benign tumors of the adrenals that are composed of hematopoietic tissue (myelo-) and fat (lipoma).
- Adenomas are most-common adrenal tumors.
- Myelolipmas contain MACROSCOPIC fat i.e visible fat. This can be identified either as low density on CT (approx -30 to -150 HU) or on MRI T1W images.
- Adenomas may have MICROSCOPIC fat. This may not be visible on routine CT and is detected on in and out of phase MR imaging.
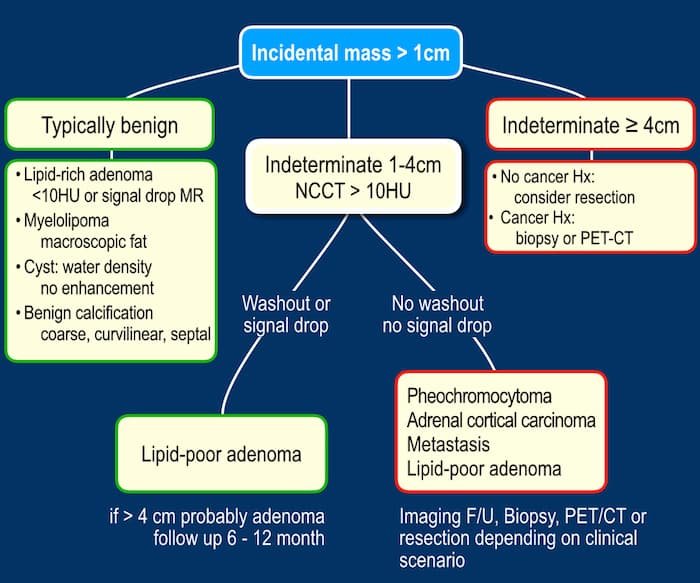
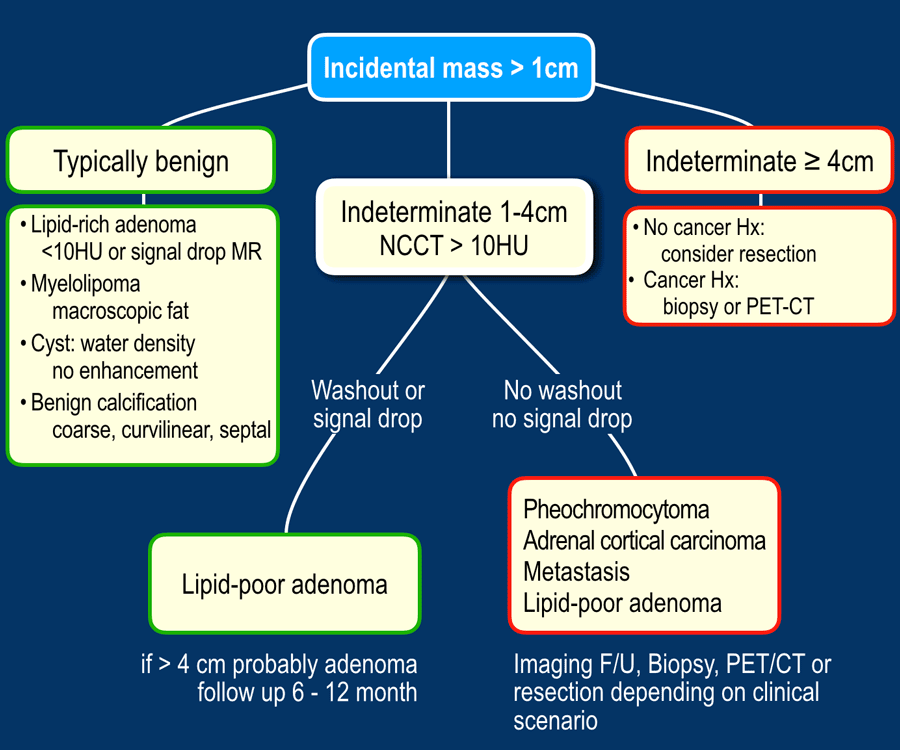
Management flow-charts for evaluation and work-up of adrenal lesions on imaging
Refer to these flow-charts by Radiology Assistant for differential diagnosis of adrenal lesion and management of incidental adrenal lesions.
References:
- Taner AT, Schieda N, Siegelman ES. Pitfalls in adrenal imaging. Semin Roentgenol 2015; 50:260–272
- Blake MA, Kalra MK, Sweeney AT, et al. Distinguishing benign from malignant adrenal masses: multi-detector row CT protocol with a 10-minute delay. Radiology 2005; 238:578-585
- Schieda N, Siegelman E. Update on CT and MRI of adrenal nodules. AJR Am J Roentgenol 2017; 208:1-12
- Radiologyassistant.nl. (2020). The Radiology Assistant: Adrenals – Lesion Characterization. [online] Available at: http://www.radiologyassistant.nl/en/p5b9ea3aca897e/adrenals-lesion-characterization.html [Accessed 29 Aug. 2019].
- [eafl id=”502″ name=”Haaga” text=”CT and MRI of the Whole Body – Haaga”]
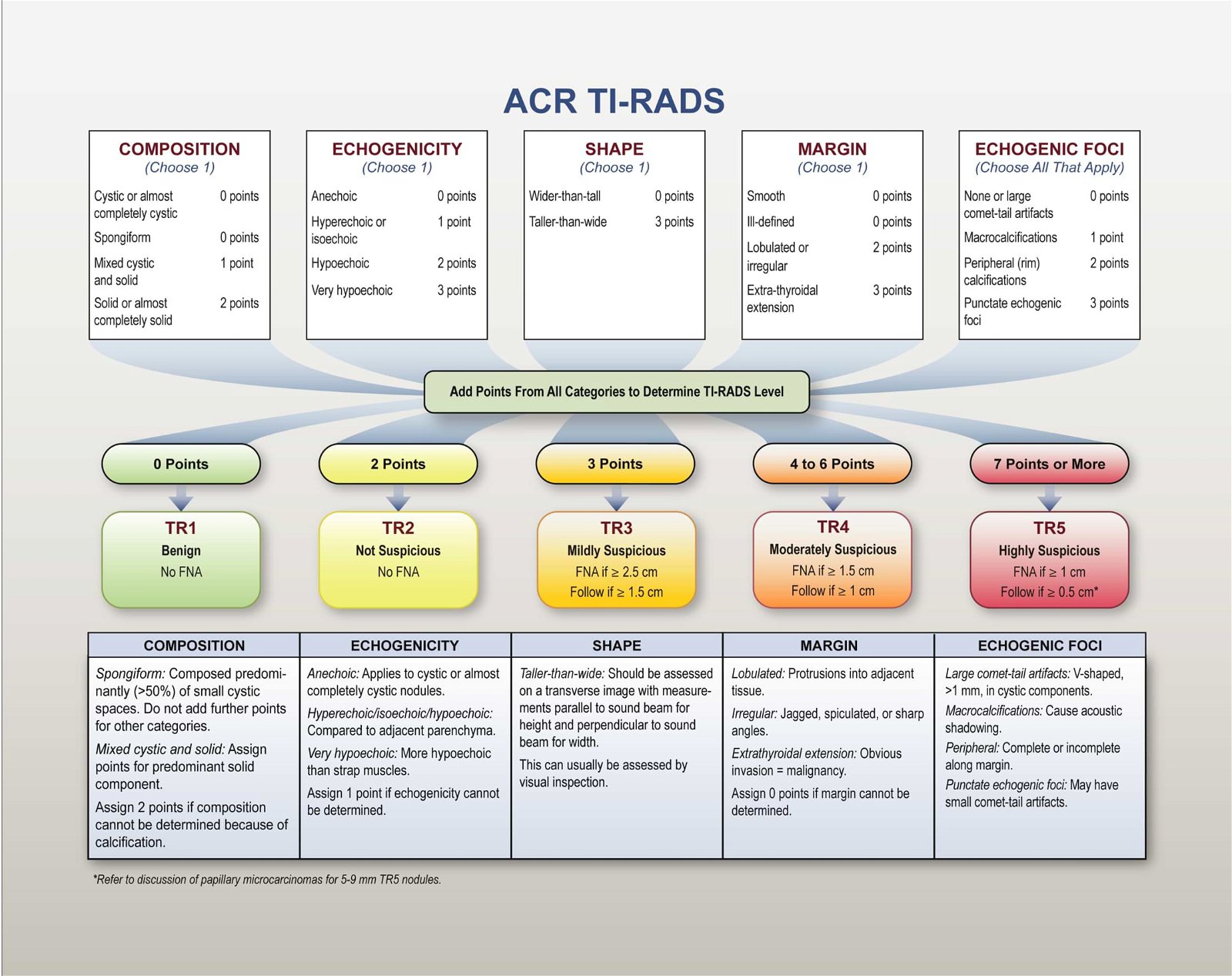
Also, check out our TIRADS calculator for thyroid nodules:
Check out other radiology calculators:
{kind=link}
Built by Dr. Amar Udare, MD
Coded by Aniket Udare

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
About the Author
Dr. Amar Udare, MD, DNB
Dr. Udare holds an MBBS and MD degree, and his expertise lies in the field of radiology. He has authored multiple peer-reviewed publications, contributing significantly to the medical field. His works can be accessed on PubMed and Google Scholar.
In addition to his academic and professional achievements, Dr. Udare is an avid reader and enjoys exploring the latest advancements in medical technology. His commitment to making complex medical knowledge accessible to patients and the general public aligns with our mission at RadioGyan.com.
For any further questions or clarifications, feel free to reach out to Dr. Udare via the contact form.