
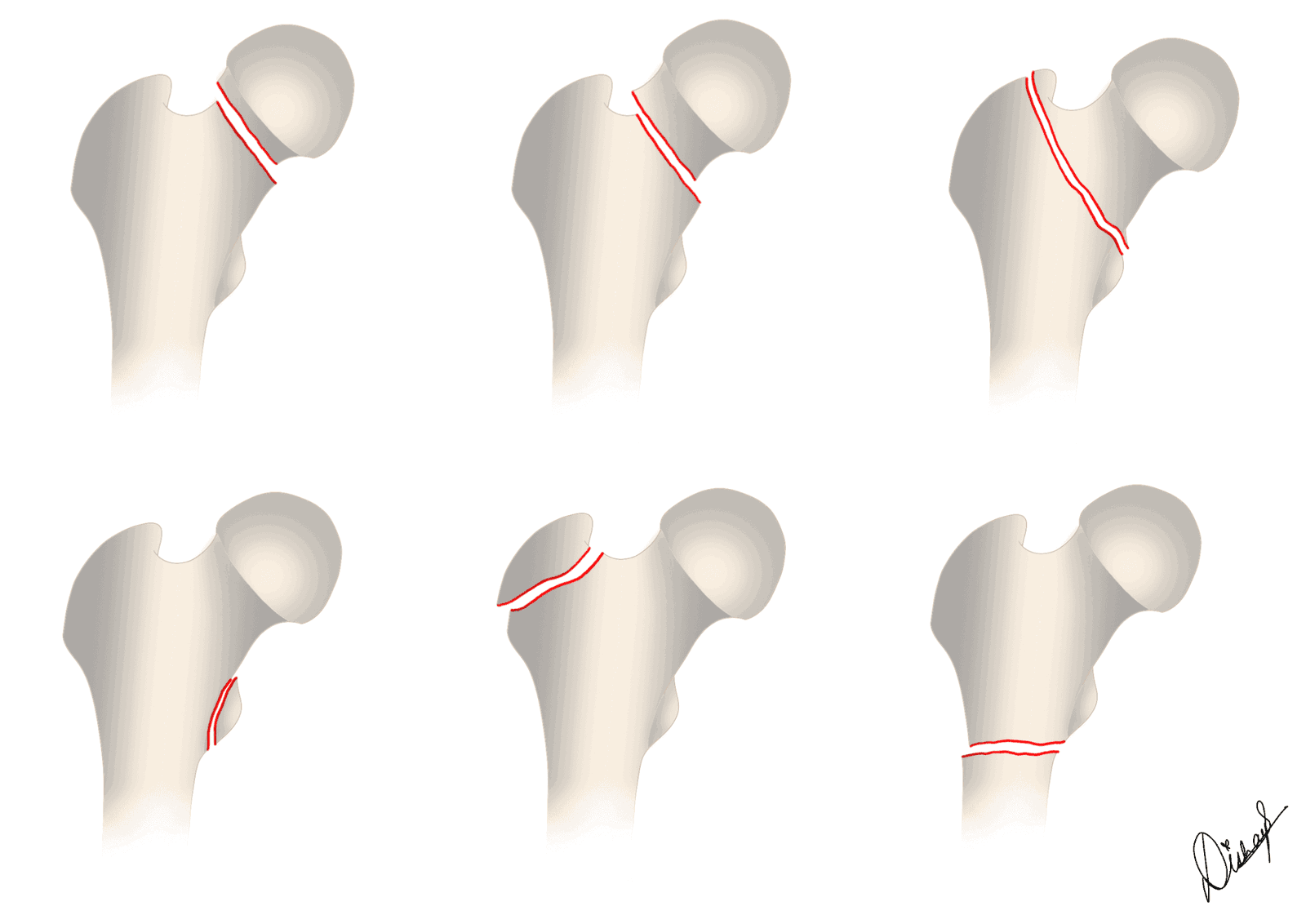
Proximal femoral fractures (“hip fractures”) are among the most common fractures the on-call radiologist reports, and the imaging findings directly drive surgical decision-making. They are grouped by anatomical level into femoral head, femoral neck (subcapital, transcervical, basicervical), intertrochanteric, and subtrochanteric fractures. The single most important distinction is whether the fracture is intracapsular or extracapsular, because this determines the risk to the femoral head blood supply and therefore the choice between fixation and arthroplasty.
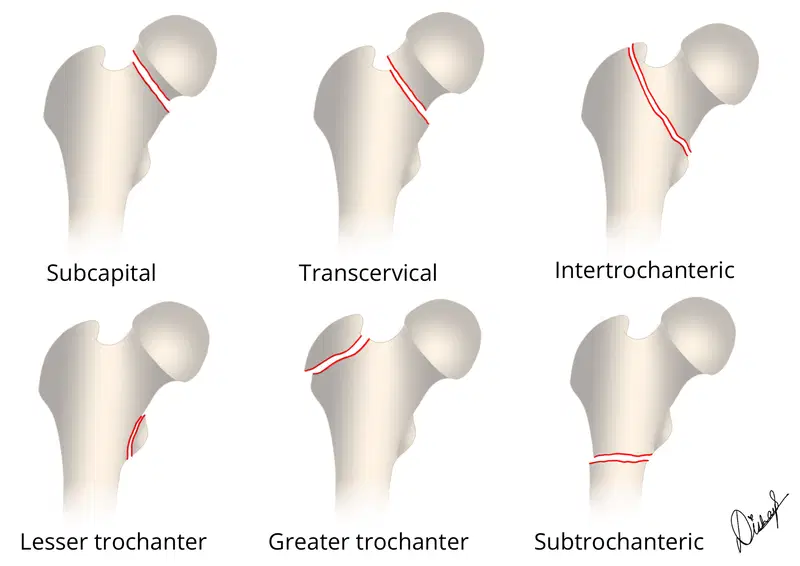
How many of these fracture subtypes can you identify? Check the labelled image at the end of the article.
Intracapsular versus extracapsular: the key distinction
The hip joint capsule attaches proximally to the acetabular rim and distally along the intertrochanteric line anteriorly and just proximal to the intertrochanteric crest posteriorly. Fractures proximal to this attachment are intracapsular and threaten the retinacular blood supply to the femoral head; fractures distal to it are extracapsular and have a robust metaphyseal blood supply, so avascular necrosis (AVN) and nonunion are uncommon.
| Subtype of proximal femoral fracture | Intracapsular or extracapsular? |
|---|---|
| Subcapital (femoral neck) | Intracapsular |
| Transcervical (femoral neck) | Intracapsular |
| Basicervical (femoral neck) | Functionally extracapsular |
| Intertrochanteric | Extracapsular |
| Subtrochanteric (within 5 cm of the lesser trochanter) | Extracapsular |
| Greater trochanter | Extracapsular |
| Lesser trochanter | Extracapsular. In an adult, consider pathological fracture |
Why does this matter? If there is one takeaway from this article, it is this. Intracapsular femoral neck fractures can disrupt the retinacular vessels (chiefly the medial femoral circumflex artery and its lateral epiphyseal branches), leading to nonunion or AVN of the femoral head. The lateral margin of the femoral head-neck junction is particularly vulnerable because it is where these vessels enter; the risk falls as the fracture line moves more distally along the neck. Management therefore aims to preserve, restore, or replace the blood supply. Basicervical and intertrochanteric fractures pose little threat to femoral head perfusion, so they are reduced and stabilised with implants that allow early mobilisation.
Femoral neck (intracapsular) fractures
Femoral neck fractures are classified by the Garden system in older patients and by the Pauwels system in younger adults. In current practice the four Garden grades are collapsed into a two-tier scheme, non-displaced (Garden I-II) versus displaced (Garden III-IV), because interobserver agreement for the individual grades is poor and management is dichotomised along exactly this line.
| Garden grade | Displacement | Description | Approx. AVN risk / typical treatment |
|---|---|---|---|
| Type I | Non-displaced | Incomplete or valgus-impacted fracture | Low AVN (about 7%); internal fixation |
| Type II | Non-displaced | Complete fracture, no displacement | Low AVN (about 7%); internal fixation |
| Type III | Displaced | Complete fracture, partial displacement (trabeculae not parallel) | Higher AVN (about 37%); arthroplasty (or urgent fixation in the young) |
| Type IV | Displaced | Complete fracture, full displacement (femoral head trabeculae realign with acetabulum) | Higher AVN (about 37%); arthroplasty (or urgent fixation in the young) |
The Pauwels classification is used in younger, higher-demand patients and describes the angle of the fracture line relative to the horizontal. A steeper (more vertical) fracture experiences greater shear force, which raises the risk of nonunion and fixation failure.
| Pauwels type | Fracture angle from horizontal | Biomechanics |
|---|---|---|
| Type I | Less than 30 degrees | Mainly compressive forces; most stable, lowest nonunion risk |
| Type II | 30 to 50 degrees | Mixed compression and shear |
| Type III | More than 50 degrees | Predominantly shear; highest nonunion and fixation-failure risk |
Although a minority of basicervical fractures are technically intracapsular, the incidence of AVN is low and they are managed as extracapsular fractures.
Femoral head fractures
Femoral head fractures are rare and usually result from high-energy trauma with hip dislocation. They are classified by the Pipkin system, based on the relationship of the fracture to the fovea and any associated femoral neck or acetabular injury.
{kind=link}
Femoral head impaction fractures may accompany anterior and posterior dislocations. A similar pattern is seen in osteoporotic patients with focal subchondral insufficiency fractures, which must be distinguished from AVN. On MRI, subchondral insufficiency fractures show a hypointense subchondral line with a large area of surrounding marrow oedema, but (unlike osteonecrosis) they consist of fracture callus and granulation tissue that enhances above and below the fracture line. AVN, in contrast, shows devascularised, non-enhancing bone and a smooth, concave, continuous low-signal line, whereas an insufficiency fracture tends to be irregular and convex toward the joint surface.
Extracapsular fractures: intertrochanteric and subtrochanteric
Intertrochanteric fractures run between the greater and lesser trochanters. The key reporting question is stability, which depends on the integrity of the posteromedial buttress (the lesser trochanter and calcar) and the presence of reverse obliquity. The Evans classification separates stable from unstable patterns; unstable configurations include comminution of the posteromedial cortex, subtrochanteric extension, and the reverse-oblique pattern.
{kind=link}
Subtrochanteric fractures occur within 5 cm distal to the lesser trochanter. The Russell-Taylor system divides them by piriformis-fossa and intertrochanteric involvement. They arise in three scenarios:
{kind=link}
- Younger patients (usually under 50) with high-energy trauma, producing comminuted fractures.
- Older patients with baseline osteoporosis and low-energy trauma, such as a fall from standing height, giving less comminuted spiral (“typical” insufficiency) fractures.
- Patients on long-term bisphosphonate therapy (over 5 years) or with impaired bone remodelling, who are at risk of atypical femoral fractures.
Atypical femoral fractures

Atypical femoral fractures (AFFs) are stress-type fractures of the subtrochanteric region or diaphysis associated with prolonged antiresorptive therapy. The radiologist plays a central role, because recognising an incomplete AFF (a focal lateral cortical lucency with periosteal beaking) can prompt drug withdrawal and prophylactic fixation before the femur completes. The 2014 ASBMR revised case definition requires the fracture to be located between the lesser trochanter and the supracondylar flare and to meet at least four of five major features, with minor features being supportive.
| Major features (at least 4 of 5 required) | Minor features (supportive) |
|---|---|
| Minimal or no trauma (fall from standing height or less) | Generalised increase in cortical thickness of the diaphysis |
| Fracture line originates at the lateral cortex and is substantially transverse | Prodromal thigh or groin pain |
| Complete fractures extend through both cortices with a medial spike; incomplete involve only the lateral cortex | Bilateral incomplete or complete fractures |
| Non-comminuted or minimally comminuted | Delayed fracture healing |
| Localised periosteal or endosteal thickening (“beaking” or flaring) of the lateral cortex | Antiresorptive or glucocorticoid use; comorbid metabolic bone disease |
Read this detailed article on atypical femoral fractures to understand why the radiologist’s role is so important:
Imaging of proximal femoral fractures
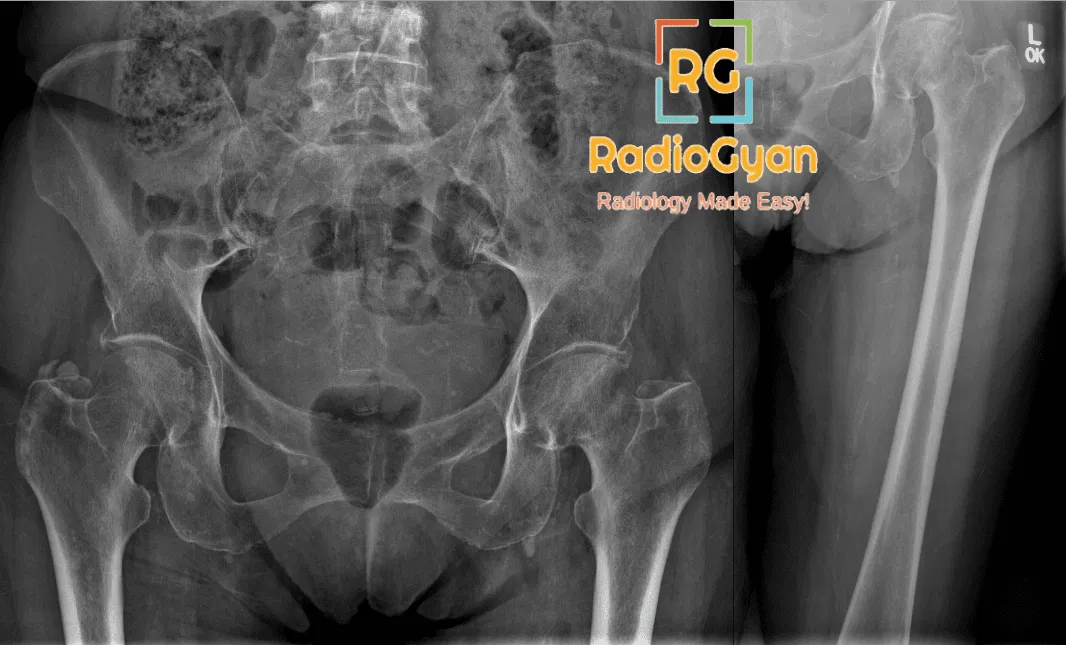
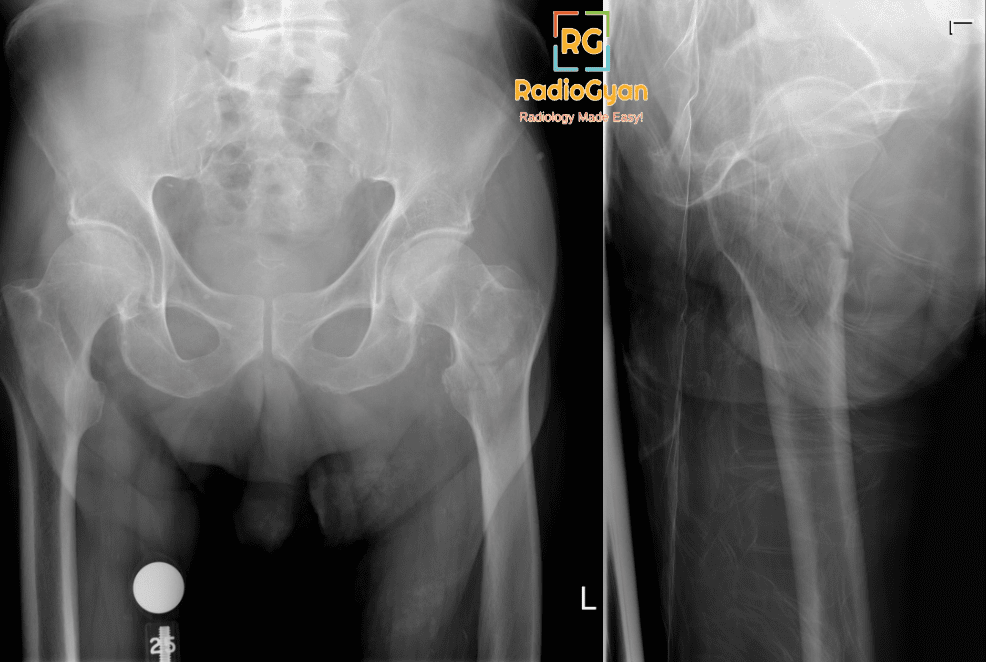
Radiographs (AP pelvis plus a cross-table or true lateral of the affected hip) are the first-line investigation. Look for a lucent fracture line, cortical step, disruption of Shenton line, and abnormal trabecular angulation. Valgus-impacted subcapital fractures are frequently missed because the only clue may be a subtle sclerotic band of impaction at the lateral head-neck junction.
Occult fractures. Radiographs can be normal in osteoporotic patients despite a genuine fracture. In a systematic review of patients presenting with acute hip pain and negative radiographs, up to about 39% had a radiographically occult surgical fracture on advanced imaging. MRI is the modality of choice and should be offered when a hip fracture is suspected despite negative radiographs; a limited coronal T1 and STIR protocol is highly sensitive and can be performed rapidly. CT is a reasonable alternative when MRI is contraindicated or unavailable, but it is less sensitive for non-displaced fractures. Trauma CT of the abdomen and pelvis often reveals an unsuspected femoral neck fracture.
MRI findings comprise a hypointense fracture line with band-like marrow oedema that is low signal on T1-weighted images and high signal on fluid-sensitive (T2 fat-saturated or STIR) sequences.
AO/OTA classification
The AO/OTA 2018 compendium codes the proximal femur as segment 31, subdivided into 31A – trochanteric (extracapsular), 31B – neck (intracapsular), and 31C – head. Each group is further split by fracture pattern and comminution. AO/OTA coding is used mainly for research and operative planning, whereas the intracapsular/extracapsular and Garden/Pauwels schemes remain the practical language of the radiology report.
Management: what the orthopaedic surgeon wants to know
Treatment is driven by the fracture location, displacement, and the patient’s age and pre-injury function. All hip-fracture patients benefit from orthogeriatric co-management, early surgery (within 24 to 48 hours), tranexamic acid, and venous thromboembolism prophylaxis, as emphasised by the AAOS 2021 and NICE CG124 guidelines.
| Fracture | Preferred treatment |
|---|---|
| Intracapsular, non-displaced (Garden I-II) | Internal fixation (cannulated screws or sliding hip screw) |
| Intracapsular, displaced (Garden III-IV), older patient | Arthroplasty with a cemented stem; total hip replacement if independently mobile, cognitively intact, and medically fit, otherwise hemiarthroplasty |
| Intracapsular, displaced, younger / high-demand patient | Urgent anatomical reduction and internal fixation to preserve the native head |
| Stable intertrochanteric | Sliding (dynamic) hip screw |
| Unstable intertrochanteric or reverse-oblique | Cephalomedullary (intramedullary) nail |
| Subtrochanteric | Long cephalomedullary nail |
Two landmark trials shape current fixation and arthroplasty choices. The HEALTH trial (NEJM 2019) found that among independently ambulating patients aged 50 or over with a displaced femoral neck fracture, total hip arthroplasty offered only a small, clinically minor advantage over hemiarthroplasty in function and quality of life, with no significant difference in secondary hip procedures at 24 months. The FAITH trial (Lancet 2017) showed no overall difference in reoperation between a sliding hip screw and cancellous screws, although smokers and those with displaced or basicervical fractures may do better with a sliding hip screw. NICE and AAOS both recommend cemented stems for arthroplasty.
Key teaching points
- Always state whether a femoral neck fracture is intracapsular or extracapsular and whether it is displaced or non-displaced: these two facts drive the operation.
- The lateral head-neck junction is the critical zone for the retinacular vessels; fractures here carry the highest risk of AVN, and the risk decreases more distally along the neck.
- Valgus-impacted subcapital fractures are easily missed; look for the sclerotic lateral impaction band.
- Negative radiographs do not exclude a fracture. If clinical suspicion persists, offer MRI: roughly two in five such patients have an occult surgical fracture.
- An isolated lesser trochanter fracture in an adult should be regarded as pathological (tumour infiltration) until proven otherwise, given how rare traumatic avulsion is in this age group.
- A transverse lateral-cortex fracture with periosteal beaking in a patient on long-term bisphosphonates suggests an atypical femoral fracture; examine the contralateral femur.
Frequently Asked Questions
References
- Sheehan SE, Shyu JY, Weaver MJ, Sodickson AD, Khurana B. Proximal femoral fractures: what the orthopedic surgeon wants to know. RadioGraphics. 2015;35(5):1563-1584. PMID: 26186669.
- Bhandari M, Einhorn TA, Guyatt G, et al. (HEALTH Investigators). Total hip arthroplasty or hemiarthroplasty for hip fracture. N Engl J Med. 2019;381(23):2199-2208. PMID: 31557429.
- FAITH Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017;389(10078):1519-1527. PMID: 28262269.
- Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2014;29(1):1-23. PMID: 23712442.
- Wilson RJ, et al. Use of advanced imaging for radiographically occult hip fracture in elderly patients: a systematic review and meta-analysis. J Am Acad Orthop Surg. 2020. PMID: 32633673.
- American Academy of Orthopaedic Surgeons. Management of hip fractures in older adults: evidence-based clinical practice guideline. 2021. PMID: 36200818.
- National Institute for Health and Care Excellence. Hip fracture: management. Clinical guideline CG124 (updated 2023). nice.org.uk/guidance/cg124.
Illustrations by TeamGyan member Dr. Disha Lokhandwala.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
Wow, this article breaks down hip fractures super clearly! The bit about intracapsular vs extracapsular and AVN risk makes total sense now. Definitely saving this for reference. Great job explaining complex anatomy simply.
Thank you for your kind words.