

Autosomal Dominant Polycystic Kidney (ADPKD)
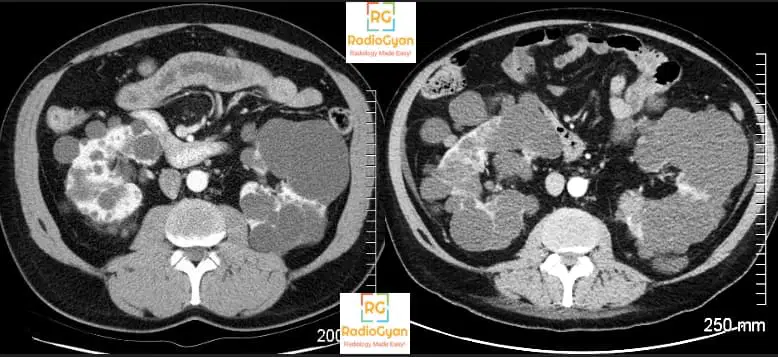
The diagnosis is pretty straightforward in this case for most of the radiologists and radiology residents. The kidneys are symmetrically enlarged with multiple cysts with a few cysts in the visualized liver as well. The radiology features are consistent with Autosomal Dominant Polycystic Kidney (ADPKD). But is diagnosis enough in this case? Is this the reason why the referring clinician has sent the patient? Read on to find out.
ADPKD introduction:
- Autosomal dominant polycystic kidney disease (ADPKD) is THE most common inherited disorder affecting the kidney and also the most common inherited cause of end-stage renal disease.
- Because it is AUTOSOMAL DOMINANT, one should always offer screening ultrasound to family members (offsprings and siblings) whenever possible. It has been found that ultrasound provides better sensitivity than genetic screening for diagnosing ADPKD.
- Associated genes on chromosome numbers 4 (PKD2) and 16 (PKD1) coding for polycystin.
- Think of ADPKD as a disorder causing weakness in the walls of body structures. So the associated systemic manifestations include :
- Cysts in other organs like liver, ovaries, spleen. seminal vesicles, prostate, and pancreas.
- Intracranial berry aneurysms – arterial wall weak. Aneurysmal rupture and subarachnoid hemorrhage can often be a presenting feature before renal insufficiency sets in. Aneurysms more than 7mm need management. Screening criteria for aneurysms in patients with ADPKD have been discussed in a recent AJNR article.
- Intracranial arachnoid cysts
- Dolichoectasia
- Colonic diverticulosis – colon wall weak.
- Aortic dissection, bicuspid aortic valve and mitral valve prolapse – Aortic wall weak.
- Clinical symptoms:
- Asymptomatic until the fourth decade when renal insufficiency develops.
- Symptoms include:
- Abdominal pain
- Hematuria
- Hypertension
- Symptoms secondary to renal failure.
Role of Imaging in ADPKD:
Ultrasound:
- Modality of choice for screening.
- Diagnostic criteria (Ravine criteria modified by Pei et al. ) for patients WITH FAMILY HISTORY.
| Age | Number of cysts |
| 15-39 years | >=3 unilateral cysts or cysts in both kidneys. |
| 40-59 years |
>= 2 cysts in EACH kidney |
| >60 years | >= 4 cysts in EACH kidney |
- Absence of cysts in patients more than 40 years rules out ADPKD.
- Ultrasound screening is recommended at 20-30 years of age, as the sensitivity is lower for patients in the younger age group.
- Typical cysts are seen as anechoic structures with posterior acoustic enhancement. Hemorrhage into cysts can produce a heterogeneous appearance. In patients with an acute presentation, it is important to assess perinephric fat as often hemorrhage can elicit an inflammatory response in the adjacent fat which is causing the patient’s symptom. A potential pitfall of ultrasound is that it can be difficult to differentiate infection from hemorrhage.
- In the patients < 15 years the recommendations for diagnosis of ADPKD are as follows as per the International consensus statement:
- USG is the screening modality of choice for ADPKD patients.
- In patients < 15 years with positive family history, one ore more cyst is suggestive of ADPKD.
- In a fetus or neonate echogenic and/or enlarged kidneys with a positive family history is suggestive of ADPKD.
- Normal USG in an at-risk patient does not rule out ADPKD.
- Multiple renal cysts with negative family history needs workup for cystic renal diseases.
- Detection of a solitary cyst in childhood requires follow-up imaging
- There are no established MRI-based diagnostic criteria for ADPKD in children younger than 15 years (evidence level B–C; recommendation level moderate).
CT and MRI:
- Not required for diagnosis in most cases.
- Ultrasound has poor sensitivity for cysts less than one-centimeter in size in infants. In these cases, T2W MRI can be used as a screening tool.
- Although renal cell carcinomas (RCC) have been reported, there is no proven association with ADPKD.
- Why patients present in the emergency setting:
- Nephrolithiasis: Non-contrast CT.
- Complex cysts (Hemorrhage or infection): CT with contrast or MRI.
Imaging to assess disease severity and progression in ADPKD:
- Total kidney volume (TKV) plays a major role in the prognosis of the disease and is the GOLD standard image biomarker for early ADPKD progression.
- Renal cysts are formed in uteri and grow with age. Up to a certain extent the renal function is preserved but in the latter phases, the cysts compress the renal parenchyma and renal insufficiency sets in. Have a look at the serial images of a patient with ADPKD a few years apart. There is progressive thinning of normal renal parenchyma on the image on the right.
- The predictive power of total renal volume has found to be better than age, genotype, serum creatinine, BUN, urinary albumin, or monocyte chemotactic protein-1 levels.
- Non contrast CT is the imaging modality of choice.
- Volume can be calculated by
- Ellipsoid formula:
- Length x breadth x-height x 0.52.
- Not very accurate but provides a rough estimate.
- More practical and a good surrogate for volumetry
- Here is a handy calculator: Radiology Volume Calculator.
- Volumetry and automated software:
- Boundary tracing on all slices and then calculating the volume.
- Precise method to measure volume.
- But is not available on all workstations.
- Ultrasound renal length (>16.5 cm)
- Ellipsoid formula:
- Height corrected Total renal volume = Renal volume/ height in meters
- A height-corrected total kidney volume (htTKV) of 600 ml/m predicts the future development of CKD stage 3 within 8 years.
- A recent study also observed that in patients with TKV > 1500 cm3, eGFR reduced at the rate of 4.3 ml/min/year.
- TKV is useful for
- Predicting prognosis.
- Monitoring response to treatment to novel drugs used for management
- Tolvaptan: vasopressin V2 receptor antagonist.
- mTOR inhibitors: Everolimus and sirolimus
- Octreotide
- Pravastatin
- Antihypertensives targeting the renin-angiotensin-aldosterone system.
- How often to measure:
- For prognosis: Once. Repeat after 1-2 years if first is inconclusive.
- For treatment response: Once every 6 months. Volumetry methods are preferred.
Differential diagnosis of ADPKD:
- Congenital disorders:
- ARPKD,
- Medullary cystic kidney disease
- Von Hippel-Lindau syndrome
- Tuberous sclerosis.
- Acquired disorders:
- Acquired cystic kidney disease (in patients with end-stage renal disease),
- Medullary sponge kidney
- Multicystic dysplastic kidney
- Localized renal cystic disease
These have been discussed in detail in this article and illustrated in these tables (Table 1, Table 2):
Conclusion:
- Ultrasound is the screening modality of choice for ADPKD.
- CT/ MRI can be used for problem solving and evaluation of complicated cysts.
- It is important to offer screening ultrasound to offsprings and siblings of patients.
- Total kidney volume is the GOLD standard image biomarker for early ADPKD progression and can be calculated on non contrast CT by using ellipsoid formula. A height-corrected total kidney volume (htTKV) of 600 ml/m predicts the future development of CKD stage 3 within 8 years.
More radiology resources on RadioGyan.com:
- Radiology resources – RadioGyan.com
- Normal Imaging Anatomy modules.: Learn and revise imaging anatomy. Links are divided by anatomy and modality.
- Cases: Radiology cases with important diagnostic points.
- Videos: Radiology videos from other websites with important teaching points highlighted.
- Spotters: Sets of 10 radiology spotters, one minute for each spotter.
- Articles: Descriptive articles on common imaging topics, including Journal club.
- Guide for first-year radiology residents.
- Guide for final year radiology residents.
- Guide to the FRCR exam
- Software: Links to common radiology software.
- Recommended Books for Radiology Residents.
- Radiology Conferences: Updates about upcoming radiology conferences and CMEs.
References and further reading:
- Renal Relevant Radiology: Radiologic Imaging in Autosomal Dominant Polycystic Kidney Disease
- Diagnostic Imaging of Autosomal Dominant Polycystic Kidney Disease.
- Imaging Approaches to Patients with Polycystic Kidney Disease
- European ADPKD Forum multidisciplinary position statement on autosomal dominant polycystic kidney disease care: European ADPKD Forum and Multispecialist Roundtable participants.
- Total Kidney Volume as a Biomarker of Disease Progression in Autosomal Dominant Polycystic Kidney Disease.
Proof checked by Dr. Iranna M Hittalamani

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case