

Quiz
Which of the following is NOT A feature of this fracture?
- Commonly extra-articular fracture.
- Volar angulation of the distal fracture fragment.
- Caused by a fall on an outstretched hand (FOOSH).
- Commonly seen in elderly women.
Pathophysiology
Colle fracture is characterized as an extra-articular fracture of the radial metaphysis caused by a fall on an outstretched hand (FOOSH), typically pronated forearm in wrist extension) causing dorsal angulation of the distal fracture fragment.
Key Imaging Features
Radiographs:
- Fracture of the distal metaphysis of the radius with dorsal angulation of the distal fragment. Often associated with ulnar styloid fracture and radial shortening.
- Signs of instability
- Dorsal tilt greater than 20°, radial inclination less than 15°, radial shortening.
- Greater than 5 mm or alternatively, resultant ulnar positive variance
- Severe comminution
- Severe displacement
- Extension into the radiocarpal joint
- Concomitant fracture of the ulna
- Age more than 60 years
- Presence of osteoporosis.
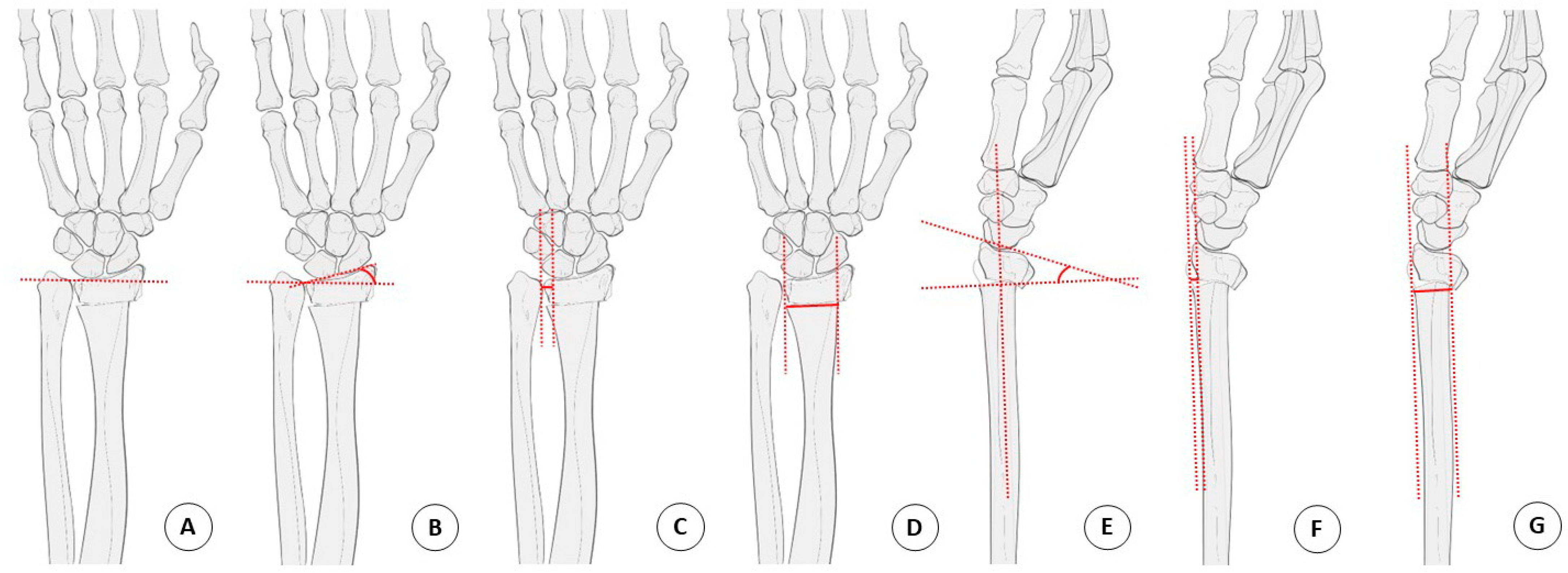
Assessment on the frontal projection:
- Radial length: Two lines are drawn perpendicular to the long axis of the radius, one at the tip of the radial styloid and the second at the ulnar border of the distal radial articular surface, normally about 12mm. Excessive shortening of the radial length is associated with injuries of the triangular fibrocartilage complex (TFCC).
- Radial inclination : Radial inclination is the angle between a line perpendicular to the central axis of the radius and a line connecting the radial and ulnar limits of the articular surface of the distal radius, normally 13-30 degrees. There is flattening of the radial articular surface in distal radial fractures.
- Ulnar variance: Vertical distance between line drawn at the level of the radial sigmoid notch and a second line at the level of the lateral cortical margin of the distal ulna. With excessive radial shortening, ulnar positive variance will be present which can lead to ulnar impaction syndromes and thinning of the triangular fibrocartilage complex. Positive ulnar variance is seen when the distal articular surface of the ulna is more than 2.5 mm distal to the articular surface of the radius.
- Radial translation ratio: The ration of the distal radioulnar joint gap relative to the radioulnar width of the proximal fracture fragment reflects the radial translation ratio. A value of more than 0.15 is a significant independent risk factor of distal radioulnar joint instability following unstable distal radius fracture.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Assessment on the lateral projection:
- Volar tilt : Angle between a line perpendicular to the central axis of the radius and a line connecting the dorsal and volar margins of the articular surface of the distal radius on the lateral view. Excessive dorsal angulation can be associated with TFCC tears.
Radiology Reporting Checklist for Distal Radial Fractures
- Is there osteopenia?
- Is there soft-tissue injury?
- Is the fracture simple or comminuted?
- Is there intraarticular (radiocarpal or distal radioulnar joint involvement)?
- Is there displacement?
- Is there abnormal dorsal or, less likely, volar tilt of the articular surface?
- Is there subluxation or dislocation of the distal radioulnar joint?
- Is there fracture of the ulnar styloid?
CT scan- in comminuted fracture to delineate fracture pattern and to rule out intra-articular component.
MRI – used to assess ligament or soft tissue injuries, such as TFCC, scapholunate or lunotriquetral ligament injuries.
Imaging Recommendation:
A radiograph with two orthogonal views (AP and Lateral ) is the investigation of choice. If there are concerns for an intraarticular fracture, CT can be obtained.
Top 3 Differential Diagnosis:
- Smith’s fracture- distal radial metaphyseal fracture caused by a fall on an outstretched hand causing volar angulation of the distal fracture fragment
- Barton’s fracture- distal radius fracture involving the dorsal aspect to the articular surface of the distal radius with intra-articular extension
- Chauffeur fractures- intra articular fracture of the radial styloid process frequently non displaced
Clinical Features:
- Symptoms: Wrist pain, swelling, and tenderness, restricted range of motion, deformed shape of the wrist
- Age/Sex predilection- Bimodal age distribution in young athletes and elderly women>men
- Risk factors – osteoporosis, a fall on an outstretched arm, athletic injuries, motor vehicle accidents.
- Complications:
- Malunion causing dinner fork deformity
- Median nerve palsy
- Post-traumatic carpal tunnel syndrome
- Secondary osteoarthritis is frequently seen in intra-articular involvement.
- Extensor pollicis longus- tendon tear
Classification System :
Frykman Classification for distal radial fractures
Based on the extra or intra-articular involvement, the fractures of the distal radius and ulna, are divided into eight different types.
| Type | Description of the fracture |
| I | extra-articular transverse metaphyseal fracture (eg- Colles and Smith’s fractures) |
| II | Type I + Ulnar styloid fracture |
| III | fractures involving the radiocarpal joint (eg-Chauffeur fractures, Barton fractures, and reverse Barton) |
| IV | type III fracture plus ulnar styloid fracture |
| V | transverse fracture involves distal radioulnar joint |
| VI | type V + ulnar styloid fracture |
| VII | comminuted fracture with the involvement of both the radiocarpal and radioulnar joints |
| VIII | type VII + ulnar styloid fracture |
The fracture is named after an Irish surgeon, Abraham Colles, who originally documented the injury in 1814 ,interestingly BEFORE the inception of radiographs.
Treatment:
1 . Extra-articular fracture with acceptable shortening (< 5 mm) and dorsal angulation ( < 5 degrees or within 20 degrees of the contralateral side)- Closed reduction and immobilization with a cast or splint.
2. Physical therapy to increase range of motion.
3. Surgical treatment options
- Closed Reduction and Percutaneous Pinning with K wires- extra-articular fracture
- Open Reduction and Internal Fixation- unstable fracture
- External fixation- open or comminuted fractures.
We discuss this fracture and other common fractures in Spotter Set 67. Access it here:
References:
Single best review article:
Other references:
Kim BS, Cho CH, Lee KJ, Lee SW, Byun SH. Pathomechanism of Triangular Fibrocartilage Complex Injuries in Patients with Distal-Radius Fractures: A Magnetic-Resonance Imaging Study. J Clin Med. 2022 Oct 19;11(20):6168. doi: 10.3390/jcm11206168. PMID: 36294489; PMCID: PMC9604910.
Co-Authors: Dr. Gauri Parvathy and Dr. Mansi Sarmalkar.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
thank you for the article
Glad you liked it.