
Quiz
What is the most common cause of rickets?
- Nutritional vitamin D deficiency
- Metabolic bone disease
- Genetic disorder
- Calcium deficiency
Key Imaging Features:
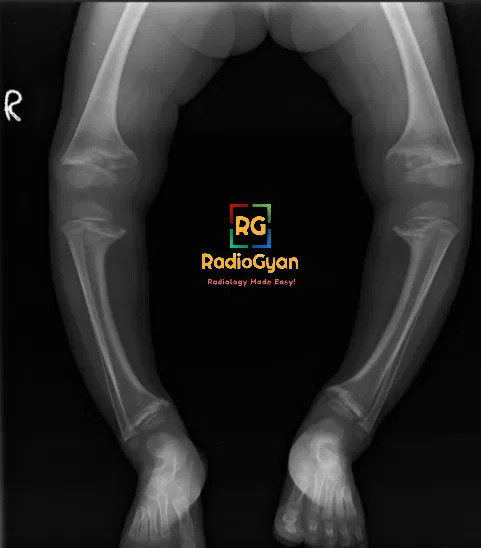
Rickets typically presents with metaphyseal cupping, splaying, and fraying at the growth plates, especially in long bones like the distal femur and proximal tibia. Loss of the thin, dense zone of provisional calcium at the physis-metaphysis interface is a hallmark feature.
- Metaphyseal Cupping: Refers to the flaring out or widening of the metaphysis, which is the wide portion at the end of a long bone where growth occurs.
- Splaying: This term describes the widening of the metaphyseal region, giving a characteristic appearance on imaging studies.
- Fraying: Seen as irregularity or roughening of the edges of the metaphysis, indicating abnormal bone formation.
- Loss of Zone of Provisional Calcium (ZPC): Typically, there is a thin, dense, well-defined zone at the interface of the growth plate and metaphysis that appears disrupted in rickets.
- Lengthening of Radiolucent Physis: The growth plate appears longer than usual due to increased unossified cartilage in affected bones.
- Most Pronounced in Long Bones: Rickets affects areas of rapid bone growth, such as the distal femur, proximal tibia, and distal radius, where these imaging features are more prominent.
Pathophysiology
Rickets occurs due to a failure to mineralize cartilage and osteoid at the growth plates in the setting of low ion concentrations, particularly calcium and phosphorus. Lack of phosphate is the ultimate problem in all types of rickets, leading to the failure of chondrocyte apoptosis and disruption of endochondral ossification.
Imaging Recommendation:
Radiographs are the primary imaging modality for diagnosing rickets. Additional imaging studies, such as MRI, may be considered in specific cases to evaluate for complications or assess bone quality.
Top 3 Differential Diagnosis:
- Newborn stress demineralization: Metaphyseal lucent bands with intact ZPC in the first 2 months after delivery.
- Metastatic neuroblastoma: Metaphyseal lucent bands with intact ZPC, often associated with osteoporosis, permeative lesions, or periosteal reaction.
- Congenital syphilis: Serrated lucent metaphyses and focal destruction of upper medial tibial metaphyseal cortex (Wimberger corner sign).
Clinical Features:
Common clinical features of rickets include short stature, genu varum (bow-legged appearance), metaphyseal swelling, pain, and fractures. Other manifestations can include craniotabes (soft bones easily indented), frontal bossing, delayed closure of anterior fontanelle, scoliosis, and rachitic rosary (palpable expanded anterior ribs).
Classification System :
There are no specific classification systems for rickets; however, it can be categorized based on underlying causes such as nutritional deficiency, genetic disorders, or metabolic abnormalities
Etymology and Synonyms:
The term “rickets” originates from the Old English word “wrikken,” meaning to twist or bend. Synonyms include “rachitis” and “vitamin D deficiency rickets.”
Treatment:
The mainstay of treatment for rickets is vitamin D therapy, often supplemented with calcium. Most cases of rickets respond well to vitamin D supplementation, leading to improved mineralization and resolution of symptoms.
References:
Single best review article:
Imaging Findings of Metabolic Bone Disease. Connie Y. Chang, Daniel I. Rosenthal, Deborah M. Mitchell, Atsuhiko Handa, Susan V. Kattapuram, and Ambrose J. Huang RadioGraphics 2016 36:6, 1871-1887
Other references:
- Aldana Sierra MC et al. Vitamin D, rickets and child abuse: controversies and evidence. Pediatr Radiol. 51(6):1014-22, 2021.
- Shore RM et al. Rickets: part I. Pediatr Radiol. 43(2):140-51, 2013.
- Elder CJ et al. Rickets. Lancet. 383(9929):1665-76, 2014.
Case submitted by Dr Vichi Goel MD Radiodiagnosis.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case