
The peritoneum is a thin serous membrane that lines the abdominal wall (the parietal peritoneum), and also covers the organs (visceral peritoneum). A thin film of fluid (about 50 to 100 mL) separates these two layers of the peritoneum from each other.
Peritoneal ligaments are double layers or folds of the peritoneum that support structures within the cavity formed by the peritoneum; Omentum and mesentery are examples of ‘named peritoneal ligaments’. Most abdominal ligaments arise from the ventral or dorsal mesentery. Peritoneal spaces are resultant separate compartments formed within the peritoneal cavity. Let us dive deeper into this.
Why is this significant?
Since the space enclosed by the peritoneum is only a potential space, normal peritoneal folds, ligaments, and thus the spaces are not identifiable at imaging. They become more conspicuous only when distended or involved by pathological processes. The peritoneal ligaments, mesenteries, and omenta may either serve as barriers for pathological processes or may facilitate the spread of disease across them.
- Identifying etiology – Infective/Inflammatory/Neoplastic/Traumatic: For eg.-Slow fluid accumulation due to a chronic underlying systemic disease may be localized to one or few spaces. The rapid build-up of fluid may suggest an acute or aggressive disease process like cases of trauma or acute pancreatitis. In such conditions, the accumulating fluid, debris, etc may not respect the natural boundaries of the peritoneal spaces and would spill into multiple spaces.
- Localizing pathology to guide the treating clinician or surgeon. For eg: for guiding placement of a drain, deciding surgical approach, etc.
- Establishing the extent of peritoneal diseases, ascites, intraperitoneal metastases, collections.
- Establishing prognosis and anticipating route of spread of disease process.
- Comparison and Follow-up.
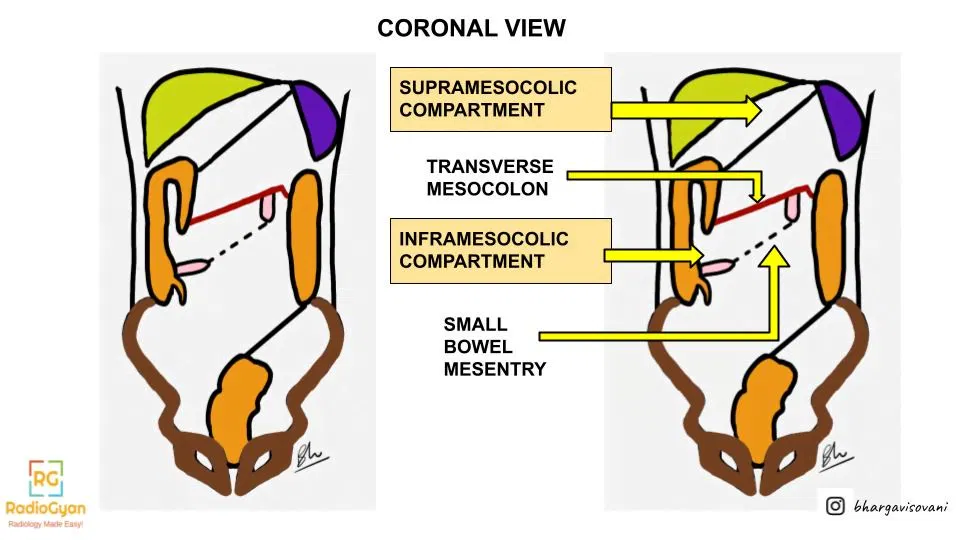
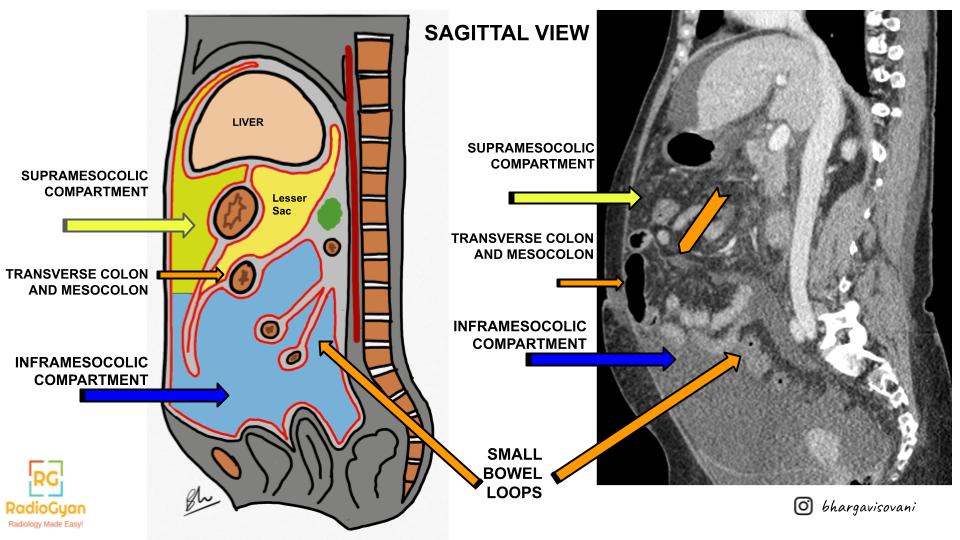
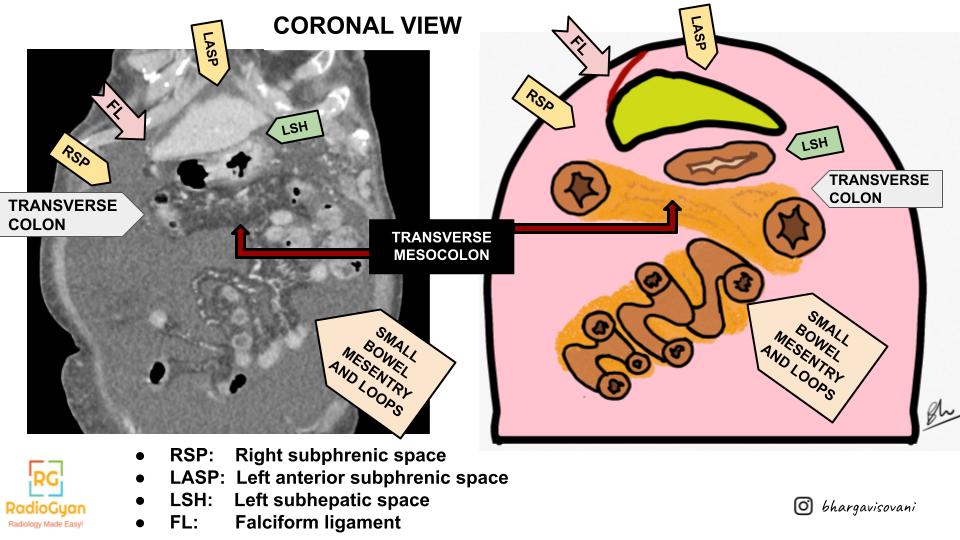
The Primary Divider – Transverse Mesocolon
The transverse mesocolon divides the peritoneum into the supramesocolic and inframesocolic spaces.
Inframesocolic space
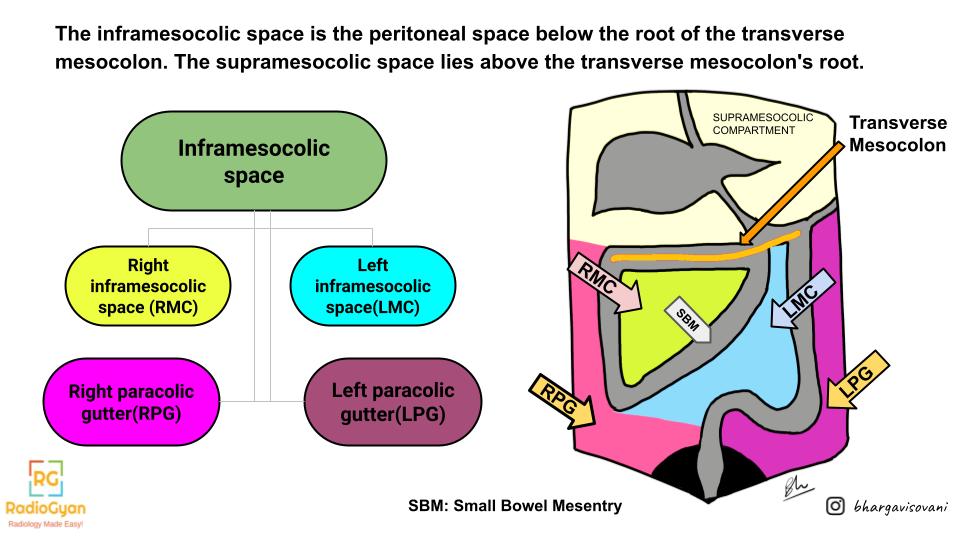
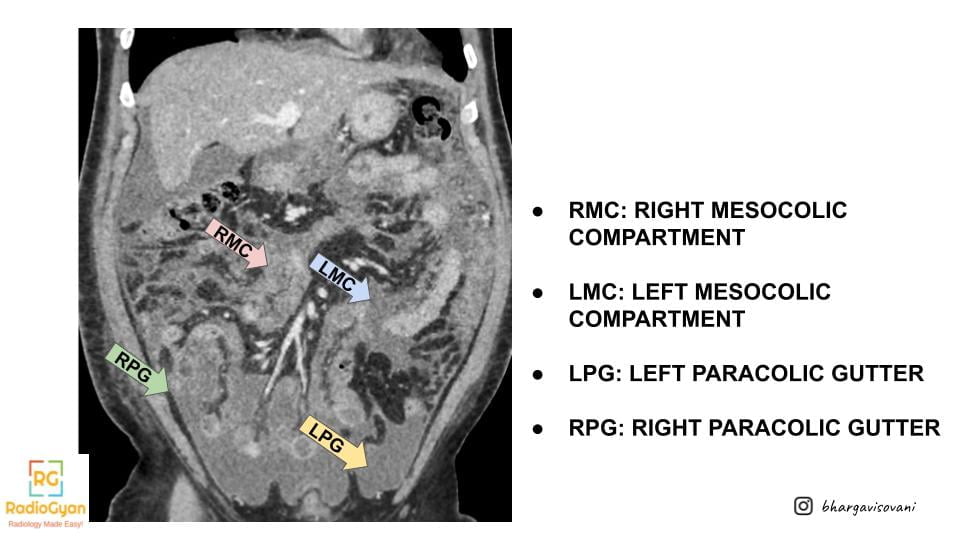
Right and Left Inframesocolic Spaces
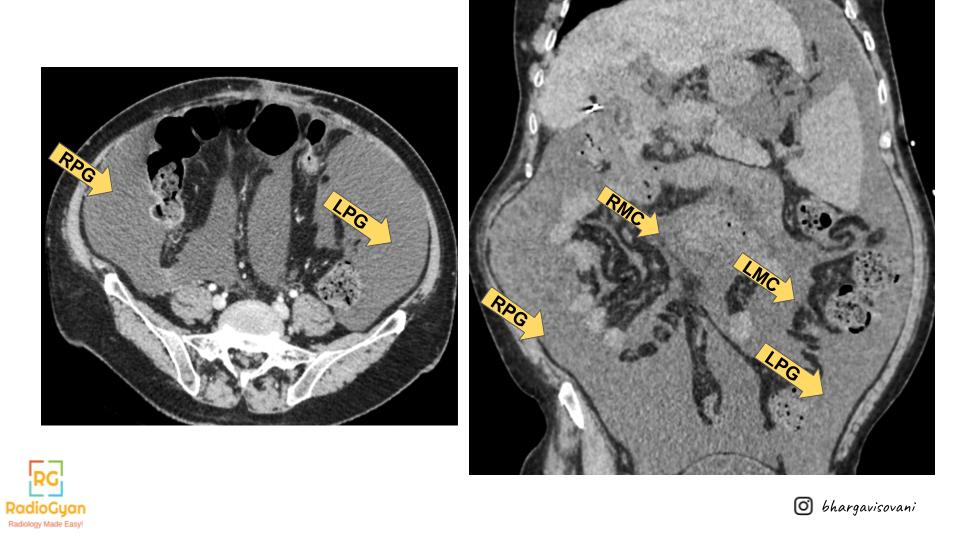
The ascending and descending colon separate the right and left inframesocolic compartments (RMC and LMC respectively) from the paracolic gutters.
The right inframesocolic space is smaller than the left and is limited inferiorly by the attachment of the small bowel mesentery to the cecum. It is for this reason that collections in this space generally do not extend into the pelvis. The left inframesocolic space is larger and has free communication with the pelvis.
Paracolic Spaces
The paracolic spaces (gutters) are located lateral to the peritoneal reflections of the left and right sides of the colon. The right paracolic gutter(RPG) is larger than the left and communicates freely with the right subphrenic space. The connection between the left paracolic gutter(LPG) and the left subphrenic space is partially limited by the phrenicocolic ligament. Both the paracolic gutters communicate with the pelvic spaces freely.
Supramesocolic space
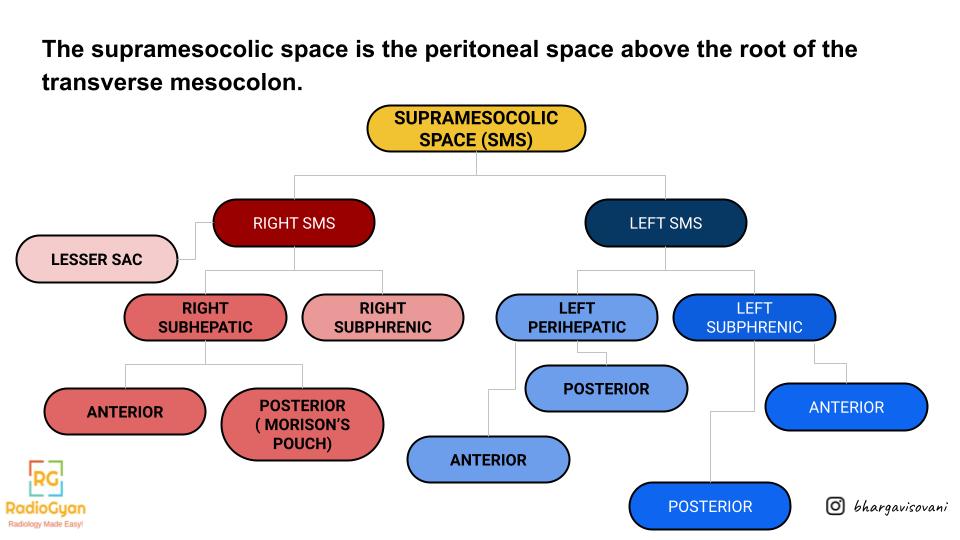
Right Supramesocolic Spaces
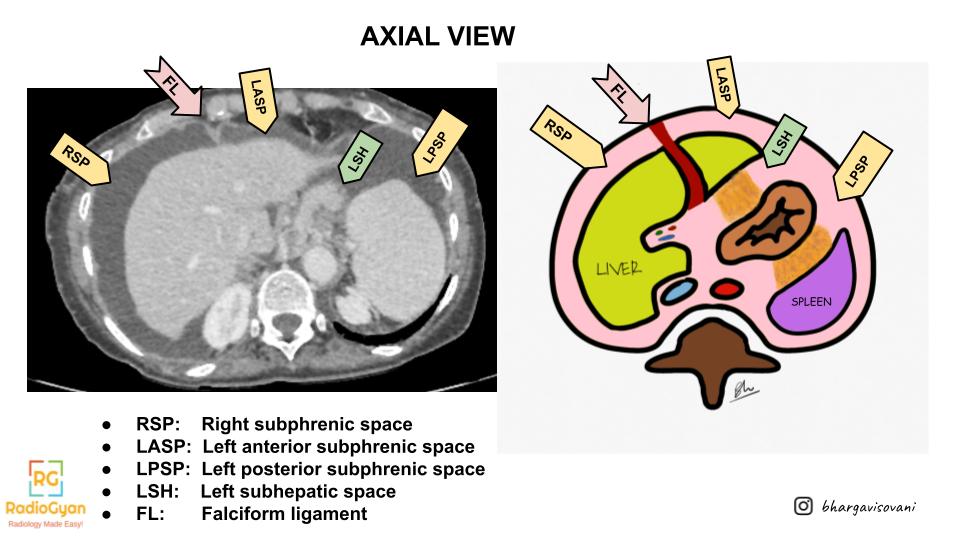
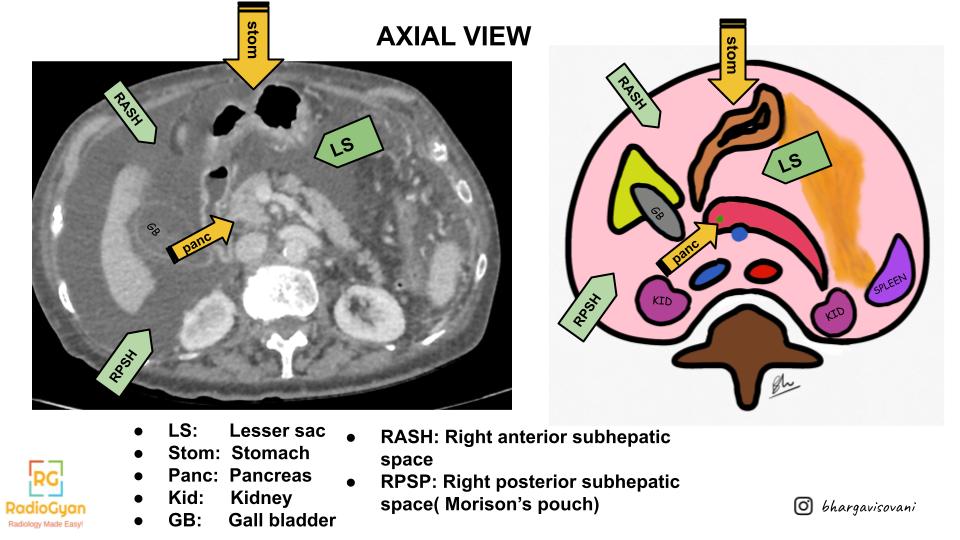
The right supramesocolic spaces include the right subphrenic space, the Morison’s pouch (subhepatic or hepatorenal space), and the lesser sac (omental bursa). The right subphrenic space is separated from the left perihepatic space by the falciform ligament, which varies in size and may not always serve as a barrier to the spread of disease
Left Supramesocolic Spaces
The left supramesocolic space includes the perihepatic, left subphrenic, and perisplenic spaces. The phrenicocolic ligament is a partial restriction to the spread of pathologic processes from the left paracolic gutter to the left subphrenic space.
Click below for more radiology articles:

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
Mam how to separate left subphrenic from perihepatic spaces. Please tell.