

Quiz
Which of the following is TRUE with regards to a ranula?
- Can undergo malignant transformation
- Most commonly congenital in etiology.
- Mucus retention cyst of sublingual or minor salivary glands
- Cyst aspiration is the treatment of choice.
Click here for the answer
Answer: Mucus retention cyst of sublingual or minor salivary glands. Read the article below to find out why the other choices are incorrect.
Pathophysiology
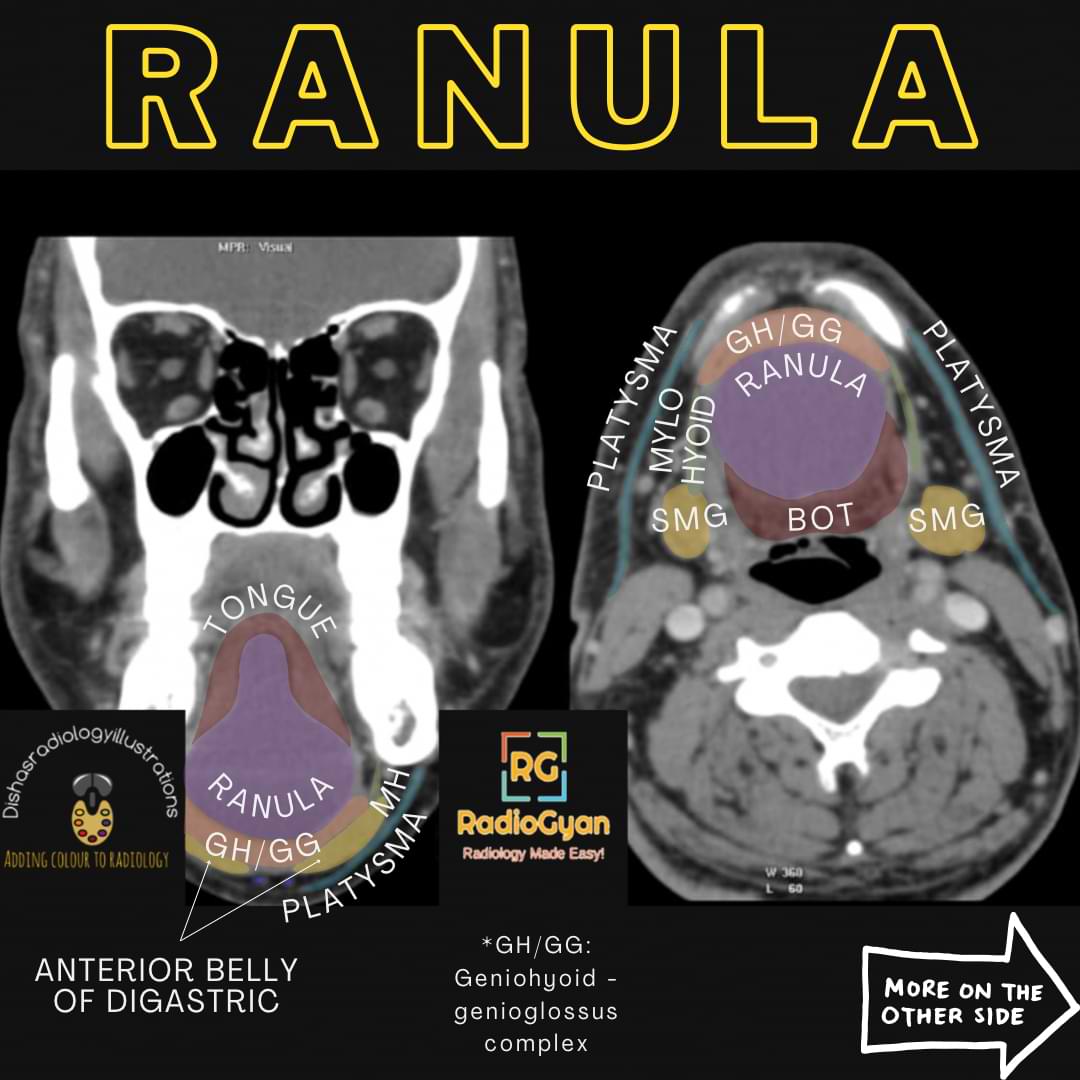
- Benign, mucous retention cyst arising from an obstructed sublingual or minor salivary glands in the sublingual space.
- Can be true cysts occurring due to ductal obstruction OR a pseudocyst resulting from ductal injury leading to extravasation and accumulation of saliva in the surrounding tissues.
- Commonly acquired and rarely congenital.
Classification System :
Ranulas are classified based on the extent of the lesion,
- Simple: confined to sublingual space. True cyst.
- Diving, AKA plunging ranula: herniated either around or through the mylohyoid muscle extending into the submandibular space. Pseudocyst.
Key Imaging Features
1. CT
1) Simple ranula- well-defined, thin-walled, unilocular, low-density cystic lesion with linear or no wall enhancement on postcontrast. Unilateral lesions appear as lenticular shapes and bilateral as horseshoe shape lesions.
2) Diving ranula-
Comet-tail morphology:
Tail sign- Collapsed sublingual portion of the cyst. All diving ranulas arise from the sublingual glands, which are seen as an extension of a small tail into the sublingual space. Lesion morphology is similar to a simple ranula with a tail in the anterior sublingual space and a body in the submandibular space medial to the submandibular gland.
3)Infected ranula-thick enhancing walls with adjacent fat stranding and content may show increased attenuation.
2. MRI
Well-defined cystic lesion with fluid signal intensity showing T1 hypointense and T2 hyperintense signal and a linear or non-enhancing wall on post-contrast studies if not infected. Altered T1/T2 signal with a thickened enhancing wall in the infectious lesion. T2 fat-suppressed sequence best delineates the tail sign of diving ranula.
3. USG
Thin-walled, hypoechoic cystic lesions in sublingual space. In case of infection, the walls appear thicker and have echogenic fluid content.
Imaging Recommendation :
Contrast-enhanced CT scan is the imaging modality of choice for the extension and characterization of the lesion.
Top 3 Differential Diagnosis :
1. Lymphatic malformation: Multilocular, septated lesion containing fluid-fluid levels and peripheral wall enhancement.
2. Dermoid and epidermoid: Low-density lesion with a thin non-enhancing wall. Fat density on CT and high signal on T1 MRI in dermoid and diffusion restriction on MRI in epidermoid.
3. Second branchial cleft cyst: Second branchial cyst can occur anywhere along the course of the second branchial apparatus, from the pharyngeal wall to the skin. The angle of the mandible is a common location. No tail sign. Branchial cysts tend to displace submandibular glands anteriorly, unlike the ranula, which displaces the submandibular gland laterally.
Clinical Features :
- Symptoms: simple ranula presents as painless swelling in the floor of the mouth, while diving ranula presents as submandibular mass displacing the submandibular gland,
- Age/Sex predilection: median age-30 years, slight male predilection.
- Risk factors: a history of neck or oral cavity trauma
Etymology and synonyms :
Ranula derives from the Latin word “Rana” meaning frog, from the resemblance of the lesion to the sublingual blebs in a frog’s mouth.

Treatment :
- Complete resection of the ranula with the obstructed sublingual gland to prevent a recurrence.
- Sclerotherapy with OK-432 and bleomycin
- Cyst aspiration has the highest recurrence rate.
References:
Single best reference article:
“Vocal Sac.” Wikipedia, Wikimedia Foundation, 8 Dec. 2022, en.wikipedia.org/wiki/Vocal_sac. Accessed 20 Jan. 2023.
“Ranula.” Wikipedia, Wikimedia Foundation, 28 Dec. 2020, en.wikipedia.org/wiki/Ranula. Accessed 20 Jan. 2023.
Co-Authors: Dr. Mansi Sarmalkar.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case