

Quiz
All the following are common features of mass-forming cholangiocarcinoma EXCEPT?
- Gradual centripetal enhancement
- Dilated bile ducts
- Liver capsular retraction
- Tumour thrombus
Click here for the answer
Answer: Tumour thrombus. Vascular encasement by mass-forming cholangiocarcinoma is common, but gross intravascular tumor thrombosis is rare, which is the differentiating feature from HCC.
Pathophysiology
Cholangiocarcinomas are malignant tumors of the biliary tract and the second most common primary malignancy of the liver after hepatocellular carcinoma. BilIN (biliary intraepithelial neoplasia,) is a precursor lesion of cholangiocarcinoma. On histology, the viable tumor cells are usually located at the periphery of the tumor. The central portion of the tumor is composed of a variable amount of fibrosis and shows coagulative necrosis with scanty scattered tumor cells which correspond to its enhancement pattern.
Key Imaging Features
- CT:
- Noncontrast and triphasic CT scan are performed.
- Homogeneous low attenuation on non-contrast scan, gradual centripetal enhancement with irregular peripheral enhancement
- Capsular retraction
- Biliary ductal dilatation
- Obliteration of the portal vein, leading to atrophy of the involved segment of the liver
- Presence of satellite nodules and vascular encasement without the formation of a gross tumor thrombus.
- Degree of contrast enhancement of the lesion depends on the degree of central fibrosis.
- MRI/MRCP: The lesion shows T2 hyperintense and T1 hypointense signal with peripheral and centripetal enhancement more prominent than at the CT scan. MRCP non-invasively evaluates the biliary tree anatomy, the status of the biliary tree proximal and distal to obstruction and accurate preoperative staging.
- USG: The lesion is homogeneously intermediate echogenicity with an irregular but well-defined margin. A peripheral hypoechoic rim due to compressed liver parenchyma and capsular retraction.
ERCP: Endoscopic retrograde cholangiopancreatography is used for diagnostic and interventional purposes including stenting of biliary stricture.
Imaging Recommendation :
CT gives better anatomic detail in illustrating vascular or extrahepatic invasion and more accurate staging while MRI shows better contrast enhancement and facilitates the detection and evaluation of hepatic parenchymal changes peripheral to the tumor. However, both modalities are equally effective.
Top 3 Differential Diagnosis :
- Hepatic abscess: An organizing abscess, commonly seen in patients with intrahepatic stone disease and shows thick enhancing walls with central cystic change, which is uncommon in cholangiocarcinoma. The early stage of an abscess may mimic a cholangiocarcinoma, serial follow-up scans and clinical and pathological correlation is useful in making the correct diagnosis.
- Hepatocellular carcinoma: HCC shows strong late arterial phase enhancement with rapid washout, appearing hypoattenuating in the portal venous phase compared to the rest of the liver. HCC is more likely to cause tumor thrombus and less likely to cause capsular refraction and biliary dilatation, which are the differentiating features from mass-forming cholangiocarcinoma.
- Hepatic metastasis from an extrahepatic tumor: The area of central necrosis shows T2 hyperintensity and T1 hypointensity, with delayed post-contrast enhancement on the hepatobiliary phase. Areas of central necrosis are not common in mass-forming cholangiocarcinoma and help in differentiating from metastatic lesions.
Clinical Features
- Age/Sex predilection– Elderly age group with a slight male predilection
- Symptoms– Asymptomatic in the early stage, presenting symptoms in the late stage of the disease include jaundice, pruritus, steatorrhoea, abdominal pain, and dark urine. Deranged liver function test, elevated CEA and Ca 19-9.
- Risk factors– Liver flukes, Hepatolithiasis (recurrent pyogenic cholangitis), Primary sclerosing cholangitis (PSC), Viral infection (HBV, HCV), Alcohol-related liver disease, cirrhosis, choledochal cyst, Caroli’s disease, environmental toxin (thorotrast, dioxin, polyvinyl chloride), Biliary tract-enteric drainage procedures.
Classification systems:
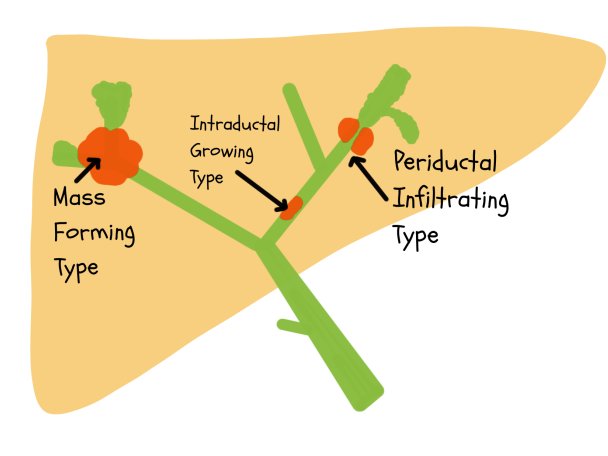
Cholangiocarcinoma is divided based on its location in the liver as intrahepatic, perihilar and distal extrahepatic. As per the liver cancer study group of Japan, intrahepatic cholangiocarcinoma is further subdivided into mass forming, periductal infiltrating and intraductal. The mass-forming subtype is most common among the intrahepatic types.
Etymology and synonyms :
The word cholangio stands for the pathology of the biliary tract and carcinoma is a malignancy arising from epithelial cells. The lesion is known as intrahepatic cholangiocarcinoma.
Treatment:
The treatment of the tumor depends on the site, extent, and staging. The definitive treatment is complete surgical resection. Palliative treatment options include stenting or surgical bypass procedures in inoperable cases.
References:
Single best review article:
Other references:
Co-Authors: Dr. Mansi Sarmalkar and Dr. Bhargavi Sovani (illustration).

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
excellent and thank you
Glad you liked it. You can check other cases here: https://radiogyan.com/radiology-cases/