
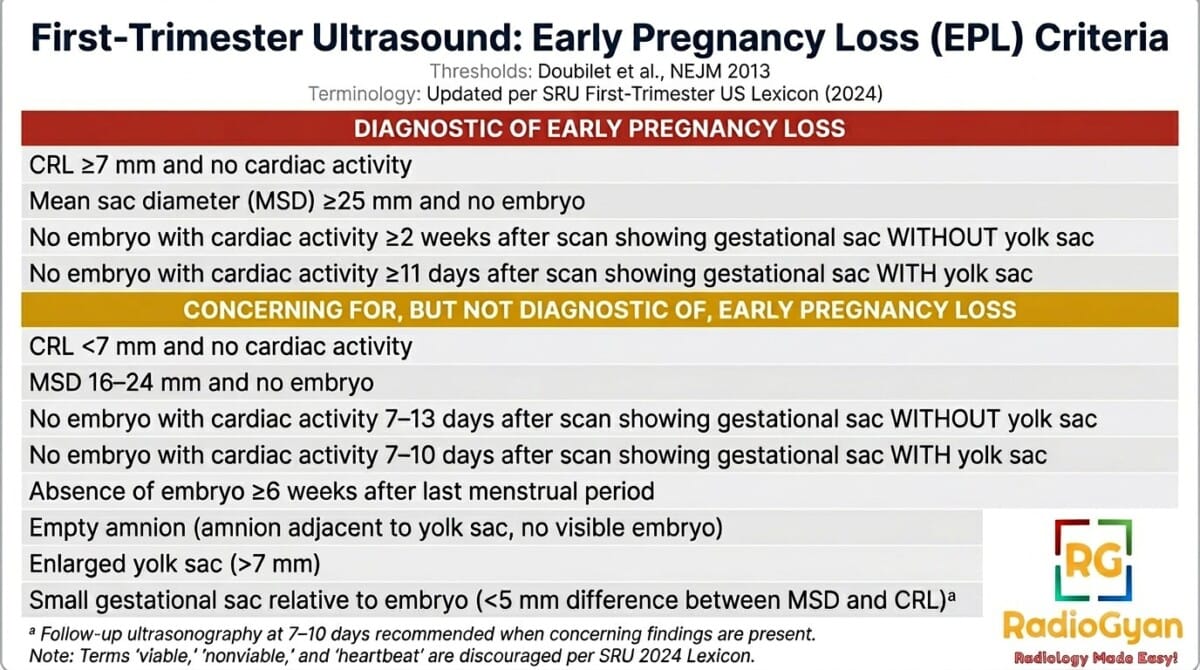
Findings Diagnostic of Pregnancy Failure
- Crown–rump length(CRL) of ≥7 mm and no heartbeat.
- Mean sac diameter(MSD) of ≥25 mm and no embryo
- Absence of embryo with heartbeat ≥2 wk after a scan that showed a gestational sac without a yolk sac
- Absence of embryo with heartbeat ≥11 days after a scan that showed a gestational sac with a yolk sac
Findings Suspicious for, but Not Diagnostic of, Pregnancy Failure
- Crown–rump length of <7 mm and no heartbeat.
- Mean sac diameter of 16–24 mm and no embryo
- Absence of embryo with heartbeat 7–13 days after a scan that showed a gestational sac without a yolk sac.
- Absence of embryo with heartbeat 7–10 days after a scan that showed a gestational sac with a yolk sac
- Absence of embryo ≥6 wk after last menstrual period
- Empty amnion (amnion seen adjacent to yolk sac, with no visible embryo)
- Enlarged yolk sac (>7 mm)
- Small gestational sac in relation to the size of the embryo (<5 mm difference between mean sac diameter and crown–rump length)
Introduction
Diagnosis and management of early-pregnancy complications, such as nonviability and ectopic pregnancy, are of utmost importance. Pelvic ultrasonography and measurement of serum human chorionic gonadotropin (hCG) levels have revolutionized the way we detect and manage these conditions. However, the misuse and misinterpretation of these tests can lead to unintended harm to potentially normal pregnancies. In this blog post, we will explore the concepts surrounding the diagnosis of nonviability in early pregnancy and the criteria used in clinical practice.
The Diagnostic Possibilities:
When a woman presents with symptoms of pain or bleeding in early pregnancy, there are three main diagnostic possibilities: a viable intrauterine pregnancy, a failed intrauterine pregnancy, and ectopic pregnancy. To aid in the differential diagnosis, serum hCG measurement and pelvic ultrasonography are commonly performed. However, it is crucial to determine the viability of the pregnancy to guide appropriate management decisions.
Diagnosing Nonviability:
The criteria for diagnosing nonviability in early pregnancy aim to eliminate false positive results. False positive diagnoses can lead to unnecessary interventions that may harm a potentially normal pregnancy. The goal is to achieve a specificity of 100%, which means a positive predictive value of 100% for nonviability. Although achieving this goal in clinical practice may be challenging, current data suggest that a specificity extremely close to 100% is feasible.
Crown-Rump Length and Mean Sac Diameter: Two primary criteria used in diagnosing nonviability are crown-rump length and mean sac diameter. Previously accepted values for these criteria have been found to be less reliable than originally thought. Recent research suggests using a crown-rump length cutoff of 7 mm and a mean sac diameter cutoff of 25 mm to minimize false positive results. These criteria yield a specificity and positive predictive value of 100%.
Time-Based Criteria: In addition to crown-rump length and mean sac diameter, time-based criteria are also considered for diagnosing nonviability. The timing of certain events in early pregnancy, such as the appearance of the gestational sac, yolk sac, and embryo with heartbeat, is accurate and reproducible. Nonvisualization of an embryo by a certain point in time can be indicative of failed pregnancy.
Diagnosing a Viable Intrauterine Pregnancy in Pregnancy of Unknown Location
When dealing with a pregnancy of unknown location, diagnosing or ruling out a viable intrauterine pregnancy is crucial. A single hCG measurement is not sufficient to reliably distinguish between viable intrauterine pregnancies, nonviable intrauterine pregnancies, and ectopic pregnancies. Therefore, additional testing, such as ultrasonography, is necessary to guide patient care decisions.
Diagnostic and Management Guidelines Related to the Possibility of a Viable Intrauterine Pregnancy in a Woman with a Pregnancy of Unknown Location
When there is no intrauterine fluid collection and normal (or near-normal) adnexa on ultrasonography:
- A single measurement of hCG, regardless of its value, does not reliably distinguish between ectopic and intrauterine pregnancy (viable or nonviable).
- If a single hCG measurement is <3000 mIU/ml, presumptive treatment for ectopic pregnancy with the use of methotrexate or other pharmacologic or surgical means should not be undertaken, in order to avoid the risk of interrupting a viable intrauterine pregnancy.
- If a single hCG measurement is ≥3000 mIU/ml, a viable intrauterine pregnancy is possible but unlikely. However, the most likely diagnosis is a nonviable intrauterine pregnancy, so it is generally appropriate to obtain at least one follow-up hCG measurement and follow-up ultrasonogram before undertaking treatment for ectopic pregnancy.
The hCG levels in women with ectopic pregnancies are highly variable, often <1000 mIU/ml, and the hCG level does not predict the likelihood of ectopic pregnancy rupture. Thus, when the clinical findings are suspicious for ectopic pregnancy, transvaginal ultrasonography is indicated even when the hCG level is low.
Conclusion
Accurate diagnosis is essential in the management of early-pregnancy complications. It is important for practitioners in various specialties involved in the diagnosis and management of these conditions to be aware of the latest guidelines and recommendations. By adopting stringent criteria for diagnosing nonviability and ensuring appropriate use of diagnostic tools, we can improve patient care and reduce the risk of harm to potentially normal pregnancies.
Reference and further reading:
Frequently Asked Questions

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case