
62 yr female presenting with progressive exertional dyspnea and palpitations.
Diagnosis and teaching points:
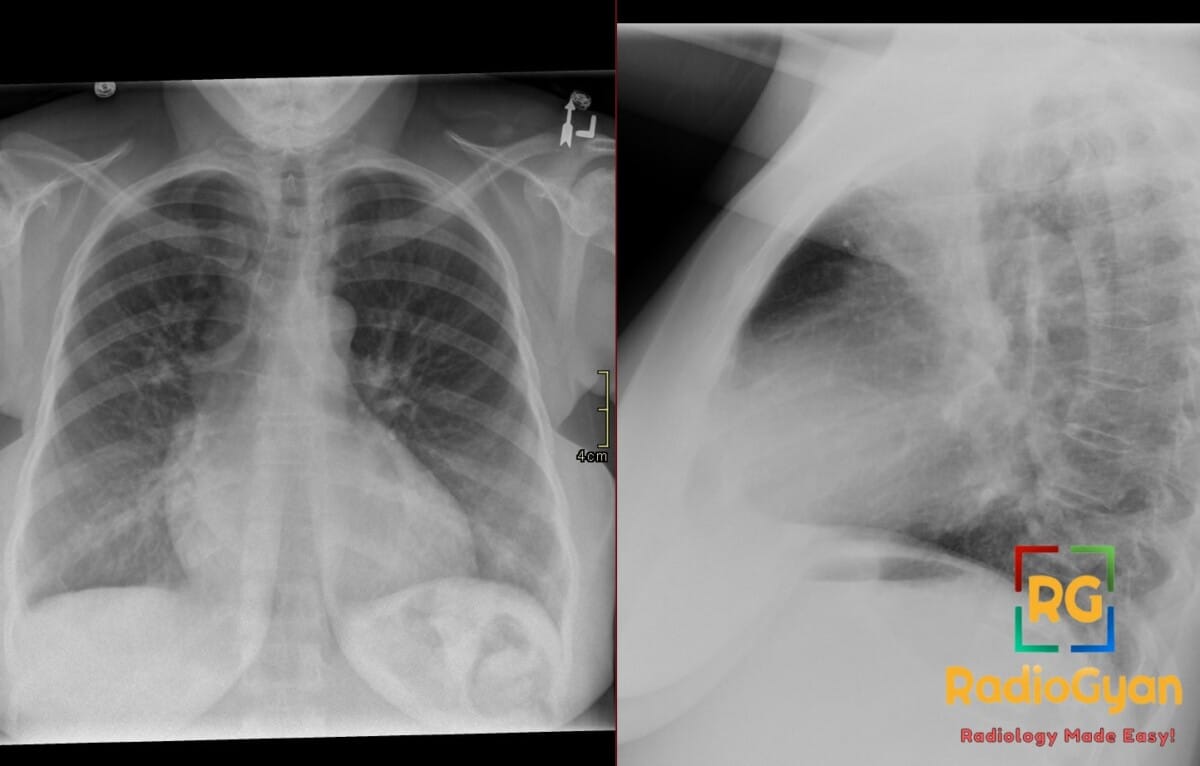
Diagnosis: Left atrial enlargement with double density sign and multiple other signs.
Key facts for boards exams:
- The double density sign is a classic frontal radiograph finding where the enlarged left atrium projects behind the right atrial silhouette to form a second right heart border.
- Splaying of the carina is characterized by a widened subcarinal angle of greater than 90 degrees due to physical elevation by the enlarged left atrium on the main bronchi.
- The third mogul sign represents an abnormal convexity or bulging along the left heart border caused by the left atrial appendage.
- The walking man sign on lateral radiograph reflects posterior displacement of the left main bronchus, which creates an inverted “V” appearance with the right bronchus.
- Echocardiography is the primary modality for confirming left atrial enlargement, utilizing the left atrial volume index as the preferred method for quantification.
Detailed teaching points:
- Clinical: Left atrial enlargement typically occurs in adults due to underlying causes such as mitral valve disease, systemic hypertension, and atrial fibrillation, presenting with symptoms like dyspnea, orthopnea, palpitations, fatigue, exercise intolerance, hemoptysis, or thromboembolic events, though it can also be asymptomatic.
- Etiology/Pathophys: Pathophysiology involves chronically increased left atrial pressure or volume overload leading to atrial remodeling and chamber dilation, as seen in mitral stenosis (obstructed blood outflow), mitral regurgitation (left-to-right volume overload), systemic hypertension, or left ventricular diastolic dysfunction.
- Radiograph: Frontal chest radiographs classic findings are the double density sign (second right heart border), an oblique left atrial measurement greater than 7 cm (distance from the midpoint of the double density to the inferior wall of the left main bronchus), bulging of the left atrial appendage (third mogul sign), carinal splaying with a subcarinal angle greater than 90 degrees, elevation or posterior displacement of the left main bronchus, posterior displacement of the esophagus, visible right side of the left atrium (atrial escape), and associated pulmonary vascular congestion.
- US: Echocardiography is the principal ultrasound modality showing increased left atrial size, with left atrial volume index (LAVI) preferred for quantification over single diameter measurements; transesophageal echocardiography is the best assessment tool for left atrial appendage thrombi.
- CT: Contrast CT demonstrates an enlarged left atrial chamber with outward bowing of the wall, mass effect on adjacent structures including posterior esophageal displacement and splaying of the bronchi, underlying etiology such as mitral valve disease, congenital shunts, or cardiomyopathy, and is useful for detecting left atrial appendage thrombi and preprocedural anatomic planning.
- MRI: Cardiac MRI demonstrates increased left atrial size and volume, atrial remodeling, and impaired contractility on cine MRI; it can identify underlying myocardial disease, quantify ventricular function and flow abnormalities, and show atrial fibrosis on late gadolinium enhancement.
- Signs: Named signs include the double density sign (second right heart border from the left atrium projecting behind the right atrium), walking man sign (inverted “V” formed by the right and left bronchi on lateral view due to posterior displacement of the left main bronchus), third mogul sign (convexity of the left atrial appendage), splaying of the carina (subcarinal angle greater than 90 degrees from atrial push), atrial escape (direct visualization of the left atrium beyond the right heart contour), and aortic-pulmonic window obliteration.
- Frameworks: Assessment on chest radiograph relies on direct and indirect signs, such as an oblique left atrial dimension greater than 7 cm; in infants and small children, bronchial compression is more useful than elevation because the double density sign is less reliable; echocardiographic quantification is standardly graded using left atrial diameter and left atrial volume index.
- DDx: Key differentials include right atrial enlargement (prominent right heart border without a double density), prominent right superior pulmonary vein (mimics double density without true enlargement), general cardiomegaly (diffuse rather than selective enlargement), pericardial or mediastinal contour abnormalities (lack carinal splaying and left atrial displacement), and left ventricular enlargement (lengthens the heart and shifts the apex inferolaterally).
- Tx: Treatment targets the underlying cause, including valve intervention or symptom control for mitral stenosis, medical management or repair/replacement for mitral regurgitation, blood pressure control for hypertension, rate/rhythm control and anticoagulation for atrial fibrillation, diuretics and guideline-directed medical therapy for heart failure, and appropriate anticoagulation for left atrial appendage thrombus.
OSCE Questions
Question: What classic radiographic sign on a frontal chest projection is characterized by a second right heart border projecting behind the right cardiac silhouette in this condition?
The double density sign.
Question: What is the name of the lateral chest radiograph sign associated with this pathology where posterior displacement of the left main bronchus creates an inverted “V” appearance?
The walking man sign.
Question: What is the preferred imaging modality and specific parameter used for the quantitative assessment and grading of this condition?
Echocardiography utilizing the left atrial volume index (LAVI).
Question: What alteration to the subcarinal angle on a frontal chest radiograph is typically associated with this pathology?
Splaying of the carina with widening of the subcarinal angle to greater than 90 degrees.
Question: What valvular pathology is a classic cause of the pressure-overload state that leads to this condition?
Mitral stenosis.
MCQ Questions
1. What carinal angle on radiography suggests this pathology?
A. Less than 45 degrees
B. Greater than 90 degrees
C. Exactly 60 degrees
D. Between 60 and 75 degrees
Answer: B. Greater than 90 degrees. Splaying of the carina with a widened subcarinal angle greater than 90 degrees is a classic sign of left atrial enlargement.
2. Which sign represents left atrial appendage outline prominence along the left heart border?
A. Double density sign
B. Walking man sign
C. Snowman sign
D. Third mogul sign
Answer: D. Third mogul sign. The third mogul sign refers to the abnormal convexity along the left heart border formed by an enlarged left atrial appendage.
3. In this pathology, what causes the “walking man sign” on lateral radiographs?
A. Posterior left main bronchus displacement
B. Anterior tracheal deviation
C. Right main bronchus elevation
D. Esophageal posterior compression
Answer: A. Posterior left main bronchus displacement. Posterior displacement of the left main bronchus due to left atrial enlargement mimics a walking man silhouette on lateral views.
4. Which echocardiographic parameter is preferred for quantifying this pathology?
A. Left atrial diameter
B. Left ventricular outflow gradient
C. Left atrial volume index
D. Pulmonary venous velocity
Answer: C. Left atrial volume index. Left atrial volume index is the current echocardiographic standard for grading left atrial enlargement.
5. What PA film measurement supporting this pathology is measured from the double-density midpoint?
A. Oblique dimension exceeding 7 cm
B. Transverse diameter over 12 cm
C. Subcarinal distance under 4 cm
D. Right border displacement over 5cm
Answer: A. Oblique dimension exceeding 7 cm. An oblique measurement greater than 7 cm from the double-density midpoint to the left main bronchus supports left atrial enlargement.
Check out more such cases:




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case