


Introduction
Early Pregnancy Ultrasound is a vital tool in obstetrics for evaluating the early stages of pregnancy. It aids in confirming the presence of an intrauterine pregnancy, assessing viability, and identifying potential complications. Understanding the normal timeline and appearances is crucial for differentiating between a healthy pregnancy and potential failures.
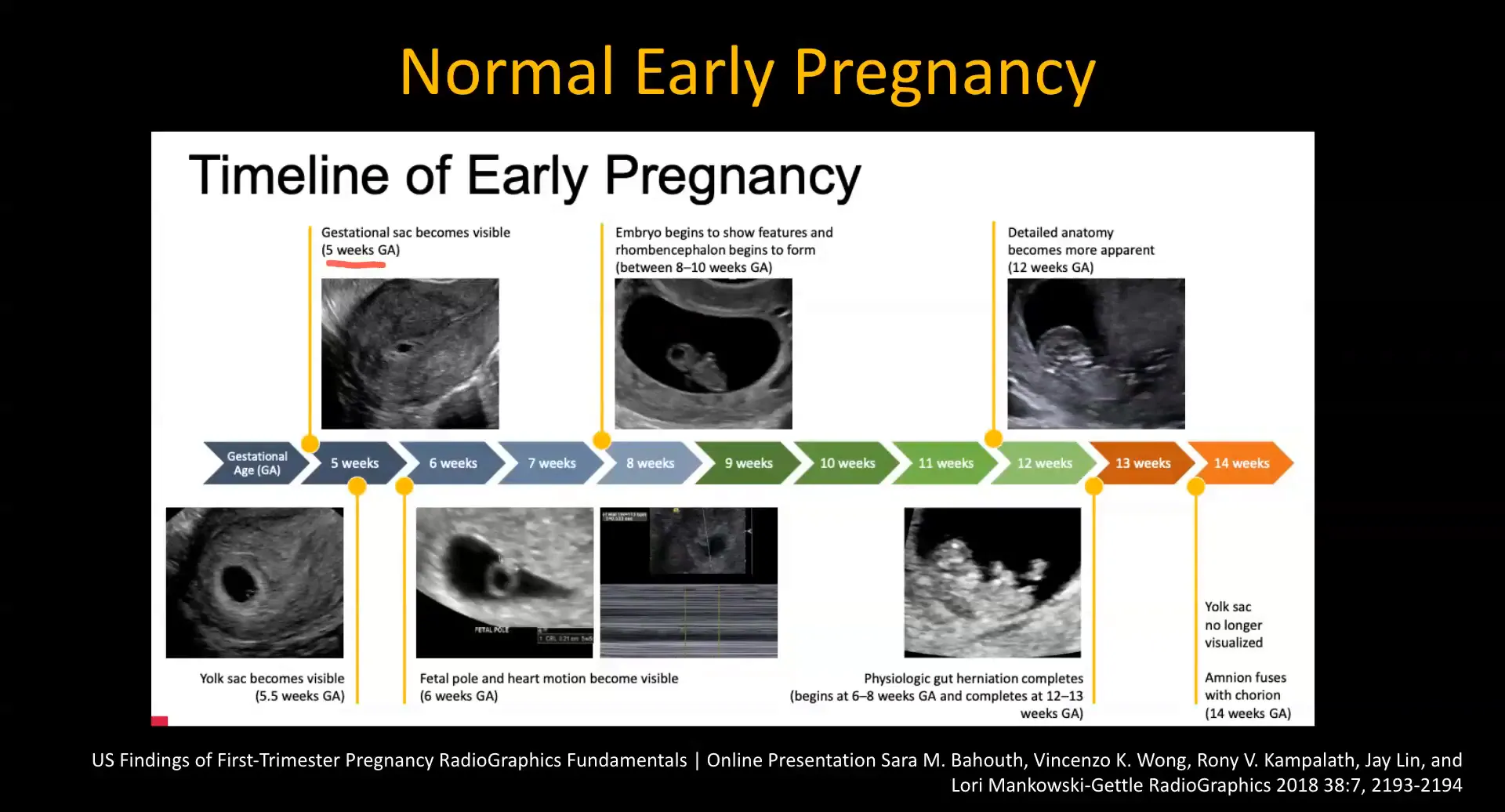
Timeline of Early Pregnancy
The early pregnancy timeline is crucial for radiologists to recognize normal versus abnormal findings. Typically, the first structure visible on ultrasound is the gestational sac, which can be identified around five weeks of gestation. Subsequently, the yolk sac appears, followed by the fetal pole, which is usually visible by six weeks.
- 5 Weeks: Gestational sac visible.
- 6 Weeks: Yolk sac and fetal pole with detectable heart rate.
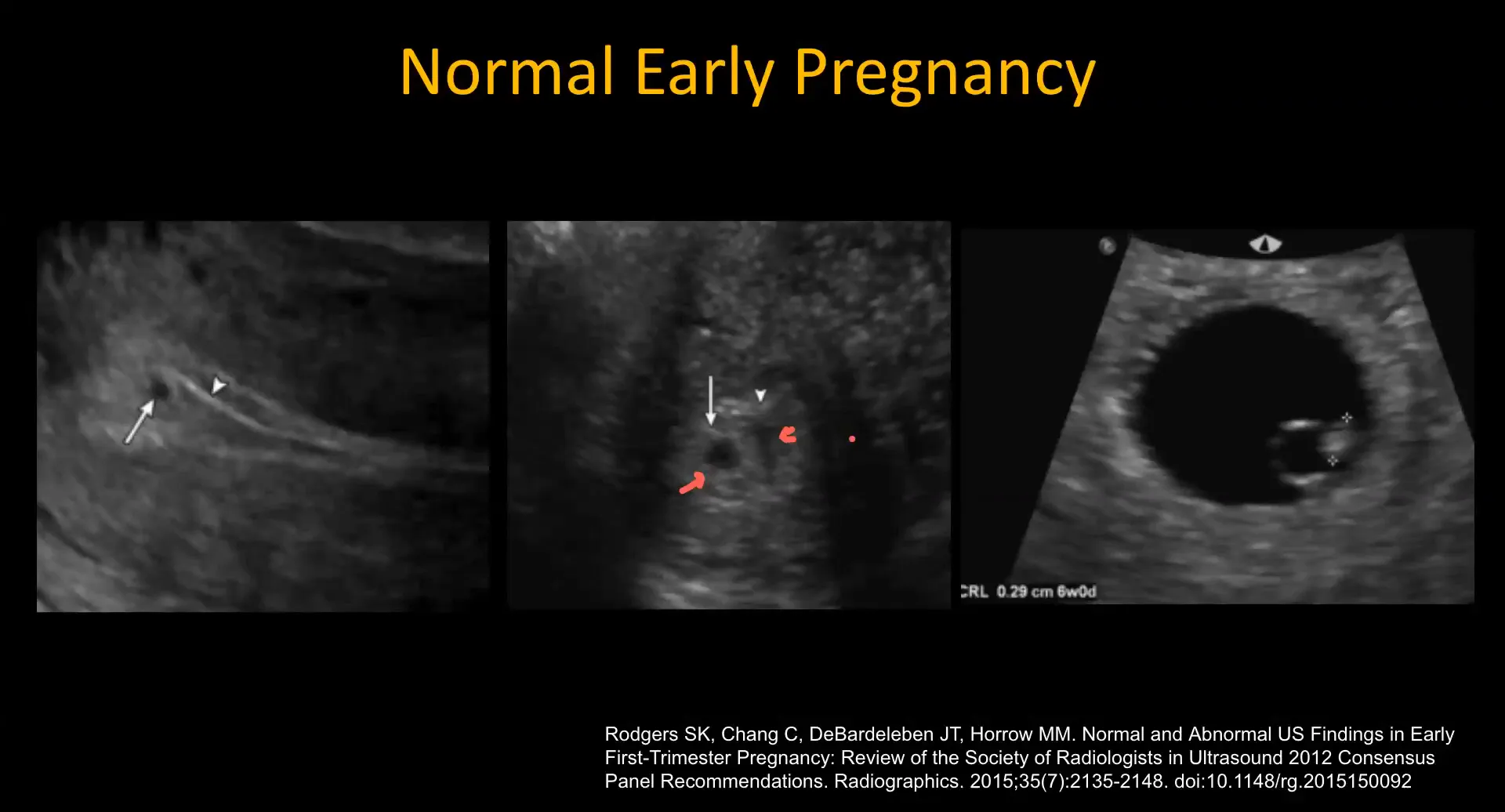
Signs of Normal Early Pregnancy
In a normal early pregnancy, several key signs can be identified on ultrasound. The intradecidual sign indicates an eccentrically located gestational sac within the echogenic decidua. Additionally, the double sac sign features two concentric echogenic rims surrounding a small fluid collection, representing the decidual reaction.
The most common normal findings include:
- Small fetal pole
- Yolk sac
- Normal-sized gestational sac
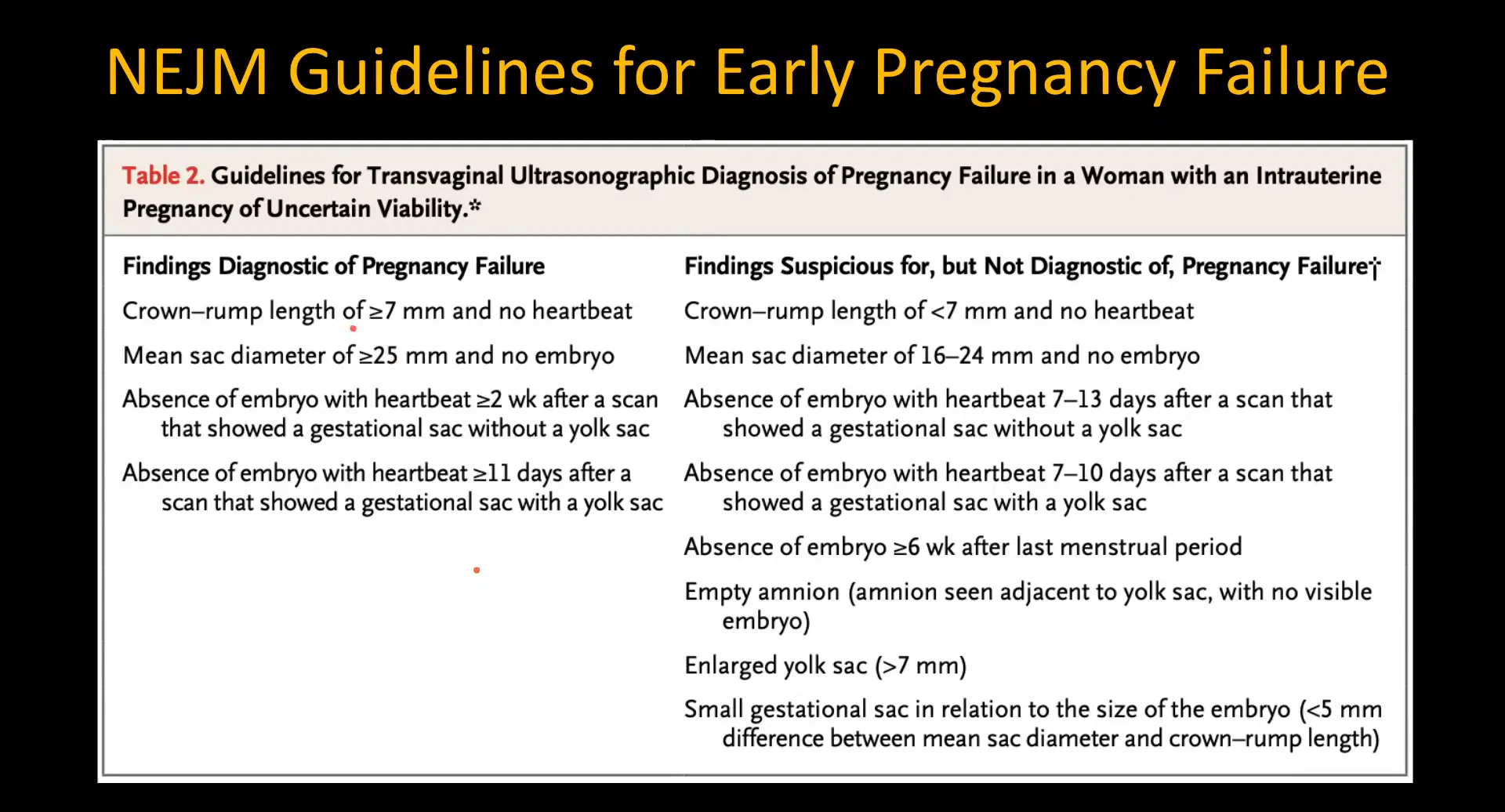
Criteria for Early Pregnancy Failure
Identifying early pregnancy failure is essential for appropriate management. The diagnostic criteria include:
- Crown-rump length (CRL) greater than 7 mm without a detectable heartbeat.
- Mean sac diameter (MSD) of 25 mm or more without an embryo.
In cases where the findings do not meet these criteria, a follow-up ultrasound is recommended after two weeks to reassess viability.
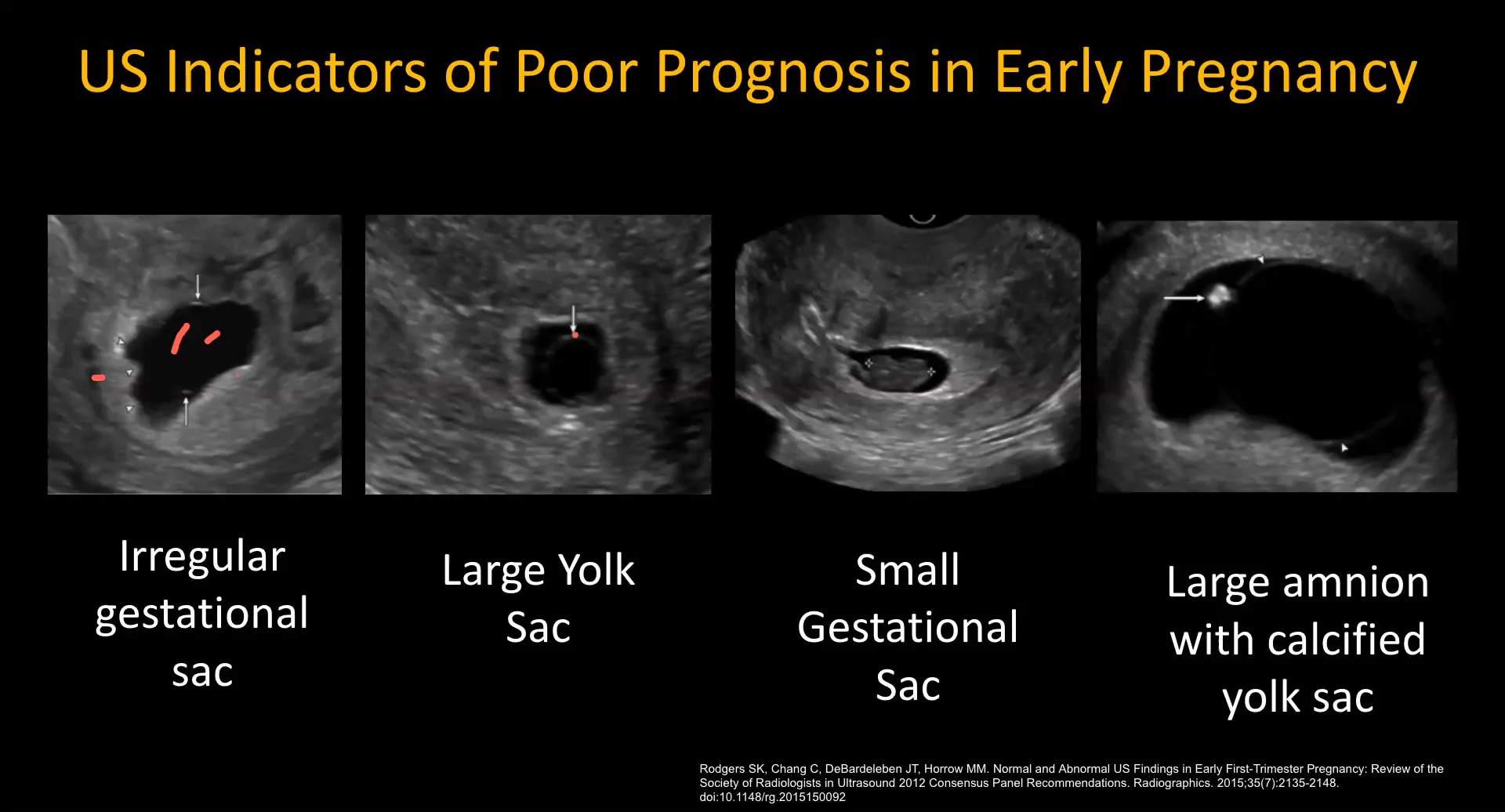
Findings Suggestive of Poor Prognosis
Several ultrasound findings may indicate a poor prognosis in early pregnancy. These include:
- Irregular gestational sac shape
- Large yolk sac (greater than 7-8 mm)
- Small gestational sac compared to fetal size
- Bradycardia (heart rate below 90 beats per minute)
- Large subchorionic hemorrhage covering more than two-thirds of the gestational sac
Recognizing these signs early can facilitate discussions with patients regarding their prognosis and necessary follow-up actions.

Terminology of Early Pregnancy Failure
Understanding the terminology associated with early pregnancy failure is crucial for effective communication in clinical practice. The terms used can often lead to confusion; therefore, clarity is essential.
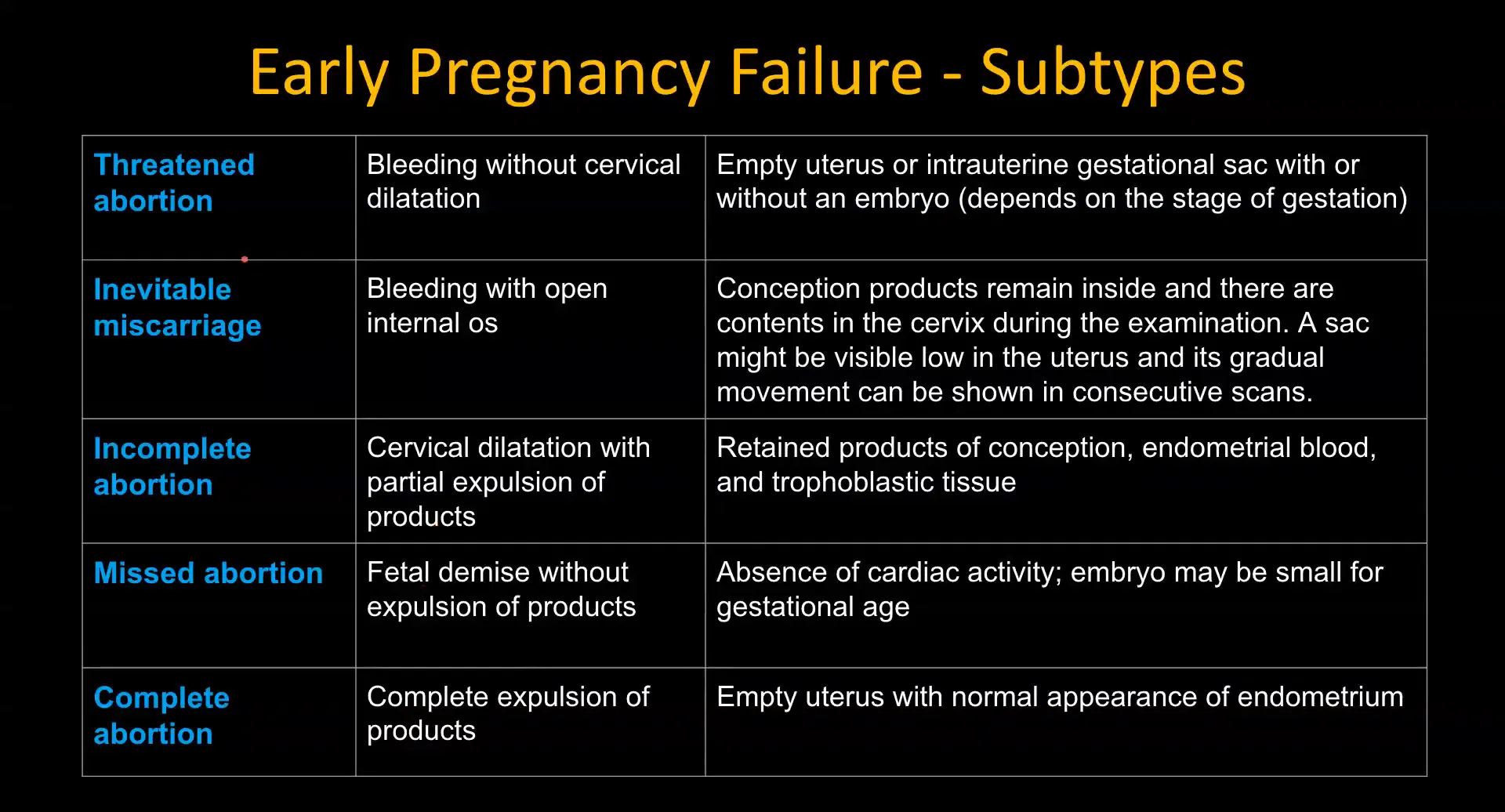
- Threatened Abortion: Refers to bleeding in early pregnancy where the cervix remains closed. Ultrasound may show an empty uterus or an intrauterine gestational sac.
- Inevitable Miscarriage: Characterized by cervical dilation with bleeding, indicating that a miscarriage is likely to occur.
- Incomplete Abortion: Occurs when there is cervical dilation with partial expulsion of products of conception, visible on ultrasound as retained tissue.
- Missed Abortion: The fetus has died but has not been expelled. On ultrasound, a gestational sac with no cardiac activity is observed.
- Complete Abortion: This is when all products of conception have been expelled, leaving an empty uterus on ultrasound.
- Pregnancy of Uncertain Viability: This term applies when findings do not confirm either a normal pregnancy or a definite failure, suggesting a follow-up ultrasound is necessary.
Retained Products of Conception (RPOC)
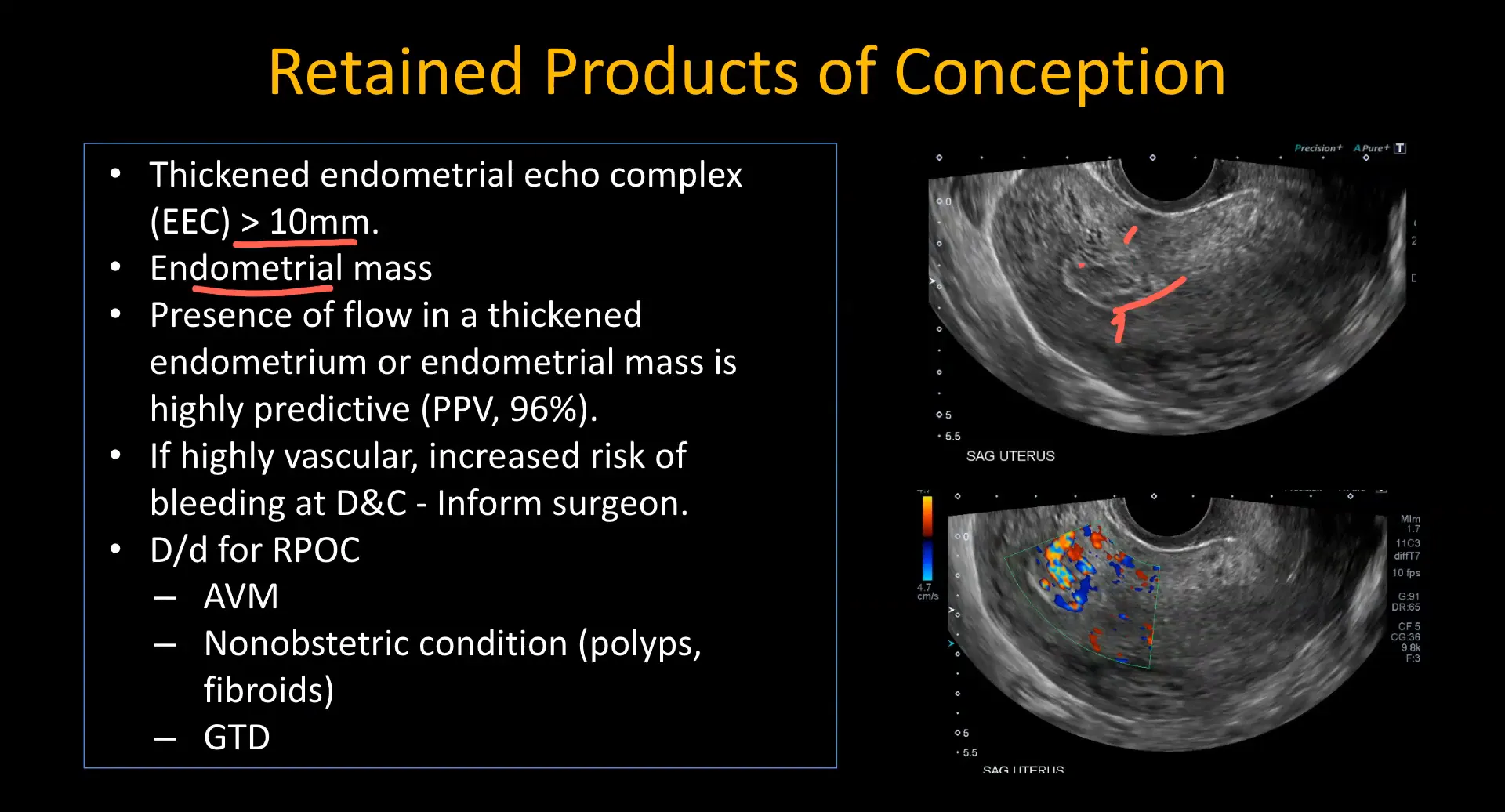
Retained Products of Conception (RPOC) can complicate recovery after a miscarriage. On ultrasound, RPOC typically presents as a thickened, heterogeneous endometrium, often measuring greater than 10 mm.
Key ultrasound findings include:
- Presence of an endometrial mass separate from the normal endometrium.
- Increased vascularity within the endometrial mass, which can be assessed using Doppler imaging.
It is essential to note the vascular characteristics, as highly vascular RPOC can lead to significant bleeding during dilation and curettage (D&C). If Doppler shows high blood flow, clinicians should be alerted to the potential for increased hemorrhage.
Differentiating RPOC from AVM
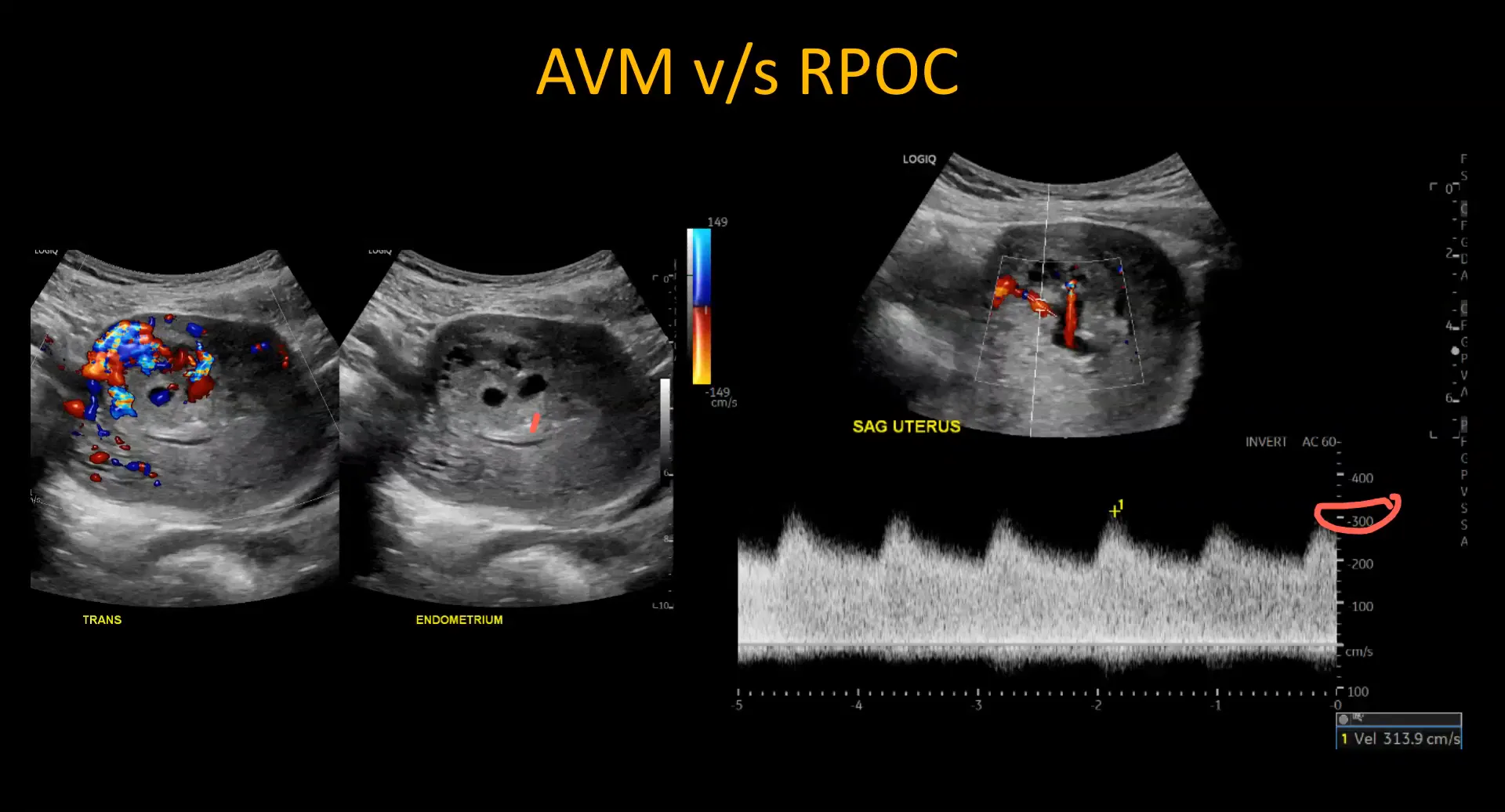
Differentiating Retained Products of Conception (RPOC) from Arteriovenous Malformations (AVMs) is crucial due to their differing management strategies. While both may present with similar ultrasound findings, key differences exist.
- Vascularity Location: In RPOC, vascularity is centered on the endometrium, whereas in AVMs, it is located within the myometrium.
- Flow Characteristics: AVMs typically exhibit very high peak systolic velocities (>200-300 cm/s) with significant diastolic flow, which is not usually seen in RPOC.
Recognizing these differences can prevent complications during surgical interventions. Doppler ultrasound is essential for accurate diagnosis.
Gestational Trophoblastic Disease
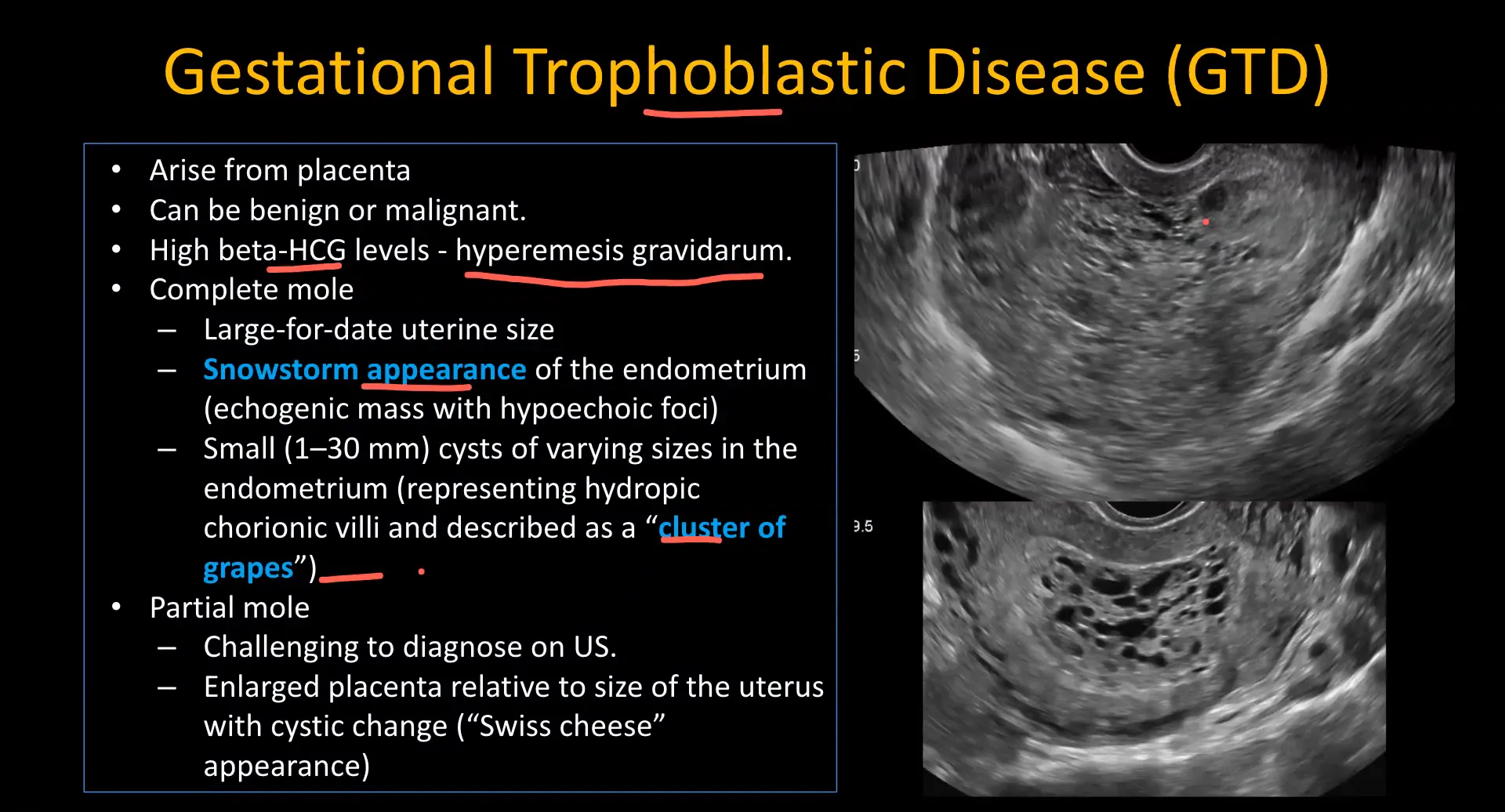
Gestational Trophoblastic Disease (GTD) encompasses a range of conditions, including complete and partial moles. These conditions are characterized by abnormal placental development and often present with elevated beta-hCG levels.
Ultrasound characteristics of GTD include:
- Snowstorm Appearance: An echogenic endometrium filled with multiple small hypoechoic foci, indicating a complete mole.
- Cluster of Grapes Appearance: Heterogeneous material in the endometrium with multiple cystic foci, indicative of partial moles.
Identifying these features is critical, as the management of GTD can vary significantly from that of normal pregnancies or early pregnancy failures. A thorough understanding of these appearances can aid in timely intervention.
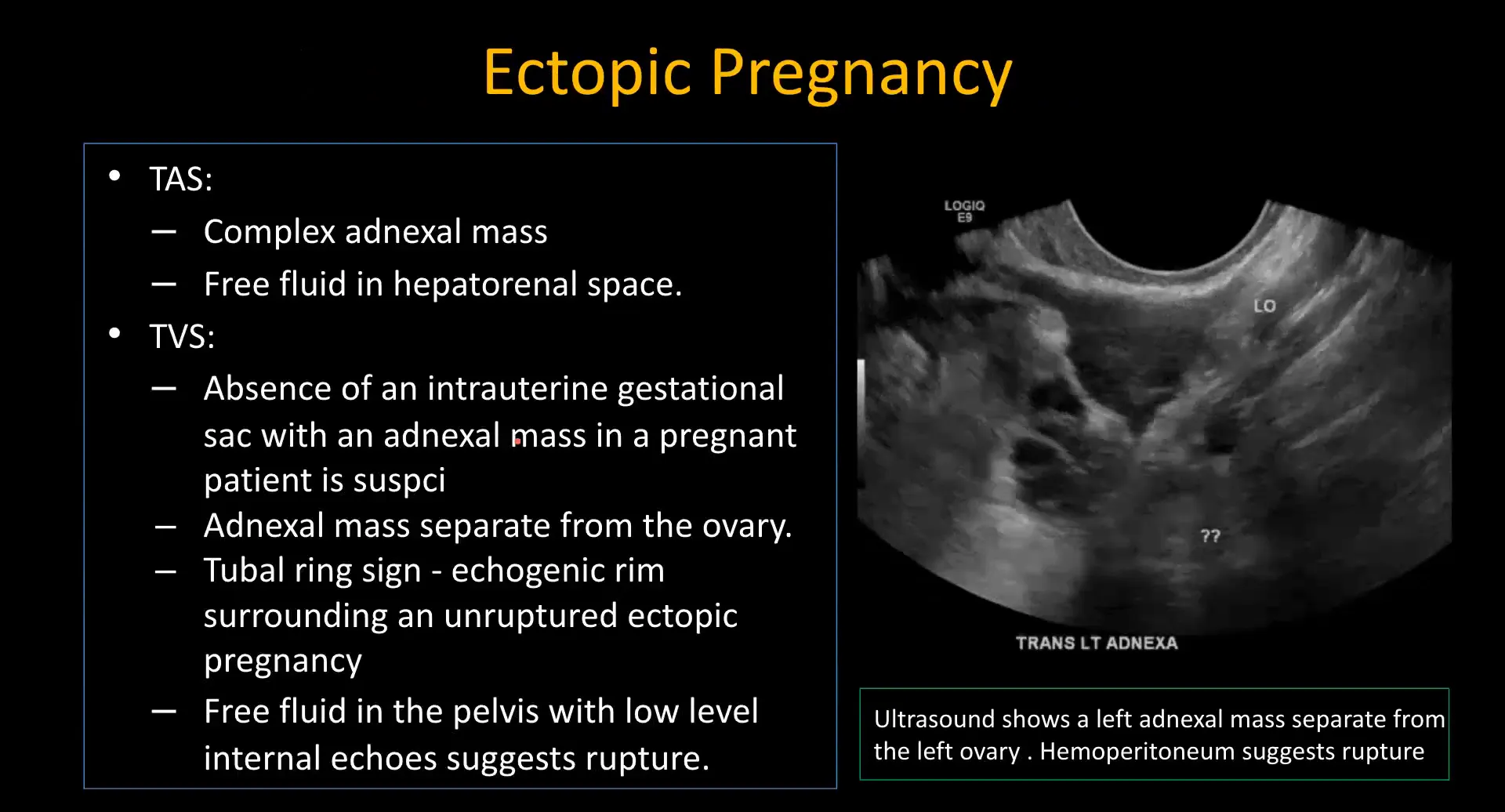
Identifying Ectopic Pregnancy
Identifying ectopic pregnancy is critical for timely intervention and management. The findings on ultrasound can be subtle, making it essential for radiologists to be vigilant.
Key ultrasound indicators of ectopic pregnancy include:
- Absence of Intrauterine Gestational Sac: If no gestational sac is observed in the uterus, further evaluation is needed.
- Presence of Adnexal Mass: A separate adnexal mass that is distinct from the ovary suggests ectopic implantation.
- Hemoperitoneum: The presence of free fluid in the abdominal cavity can indicate a ruptured ectopic pregnancy.
- Decidual Reaction: The presence of a thickened endometrium can be seen, often described as the “decidual cast.”
In clinical practice, look closely for these signs, especially in patients presenting with abdominal pain and positive pregnancy tests.
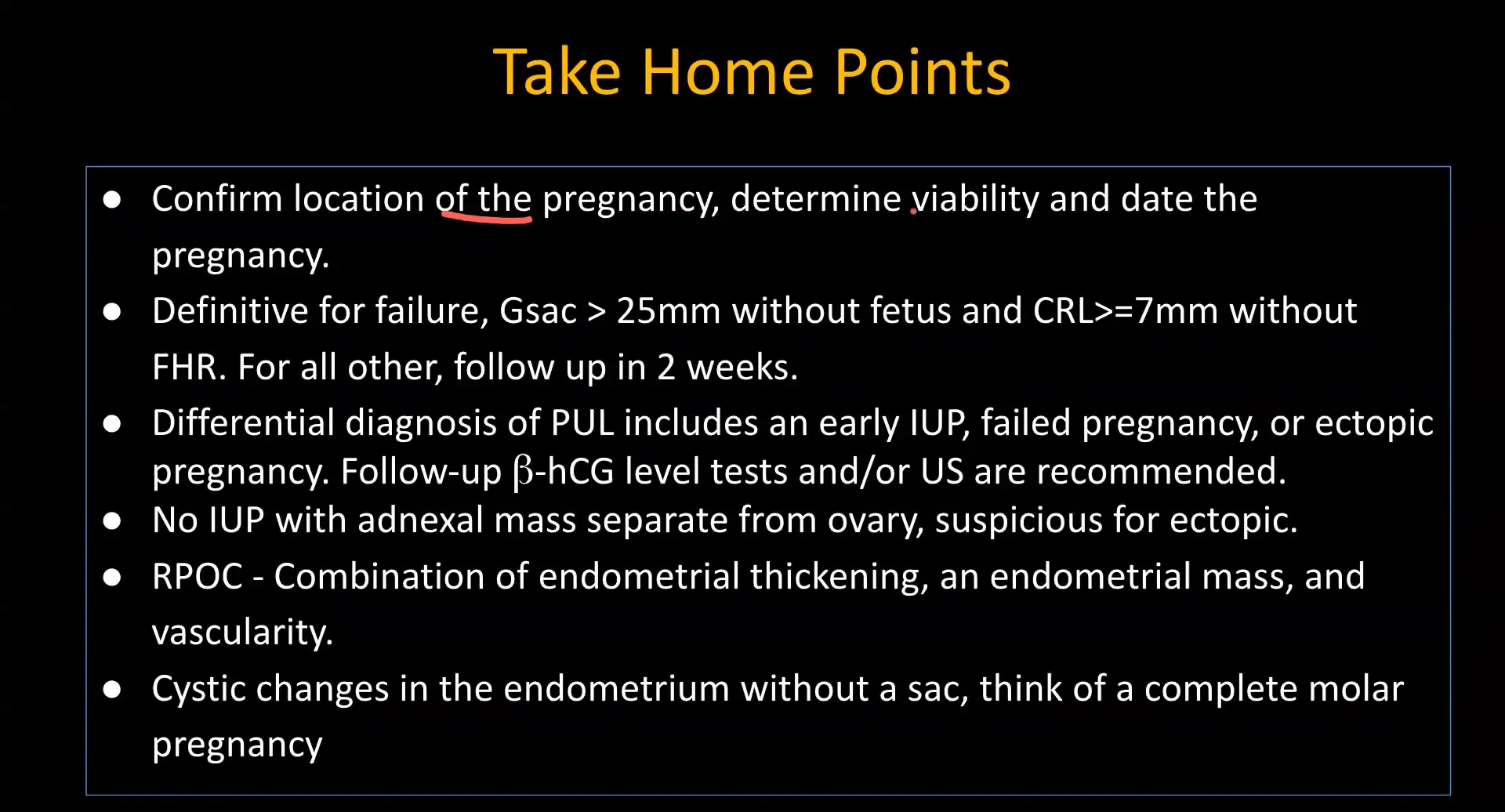
Key Points for Diagnosis
When diagnosing early pregnancy complications, including ectopic pregnancy, several key points must be remembered:
- Confirm Intrauterine vs. Ectopic Location: Always determine the location of the gestational sac.
- Evaluate Viability: Check for fetal heart activity and assess CRL (crown-rump length) and MSD (mean sac diameter).
- Timing of Follow-Up: In cases of uncertainty, a follow-up ultrasound in 1-2 weeks is crucial for reassessment.
Utilizing these points ensures a structured approach to managing potential complications in early pregnancy.
FAQs
- What are the key ultrasound findings that indicate an early pregnancy failure?
Key findings include a crown-rump length (CRL) greater than 7 mm without a detectable heartbeat and a mean sac diameter (MSD) of 25 mm or more without an embryo. - How can Doppler ultrasound assist in diagnosing retained products of conception (RPOC)?
Doppler ultrasound can assess the vascularity of the endometrial mass. Increased vascularity within the mass suggests RPOC, particularly if it shows high blood flow, indicating a risk for significant bleeding during procedures like dilation and curettage. - What differentiates an ectopic pregnancy from a normal intrauterine pregnancy on ultrasound?
An ectopic pregnancy typically presents with an absence of an intrauterine gestational sac and the presence of an adnexal mass distinct from the ovary. Additionally, free fluid in the abdominal cavity may indicate a ruptured ectopic. - What ultrasound characteristics suggest gestational trophoblastic disease?
Ultrasound findings indicative of gestational trophoblastic disease include a “snowstorm” appearance with multiple small hypoechoic foci in the endometrium for complete moles, and a “cluster of grapes” appearance for partial moles, along with elevated beta-hCG levels. - When should follow-up ultrasounds be scheduled for suspected early pregnancy complications?
Follow-up ultrasounds are generally recommended 1-2 weeks after initial assessments for cases of uncertain viability, missed abortions, or when specific criteria for early pregnancy failure have not been met.




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case