
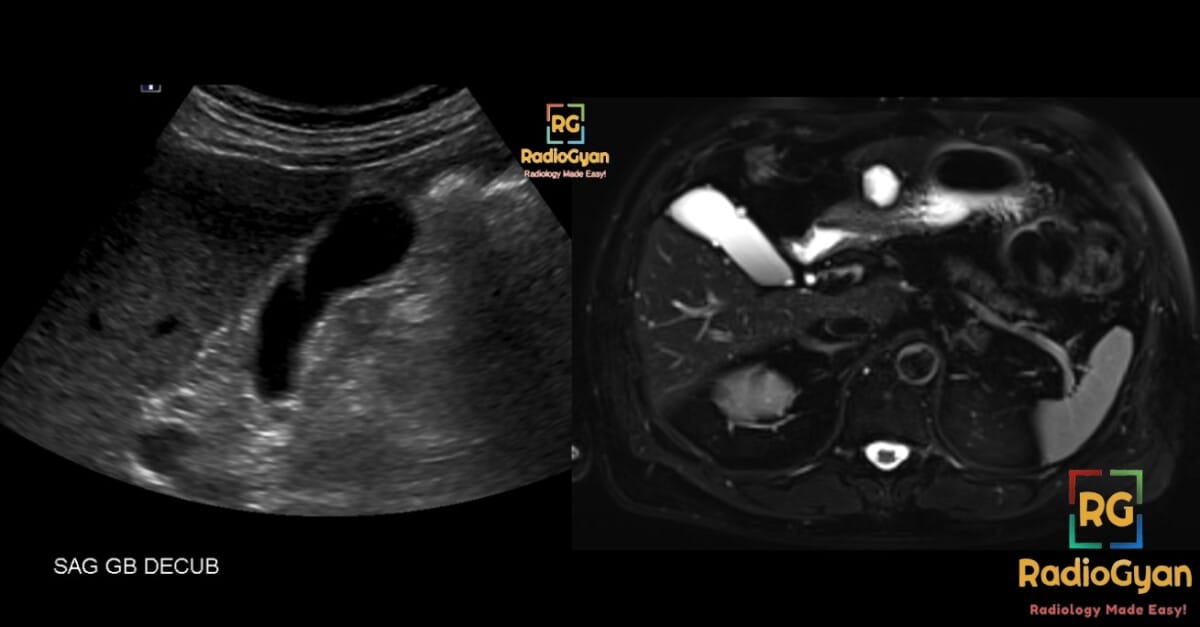
Gallbladder polyp seen on ultrasound
Short interval follow-up US within 1-2 months with optimized grayscale, color Doppler technique, and patient preparation
Short interval follow-up US within 1-2 months with optimized grayscale, color Doppler technique, and patient preparation
CEUS or MR for further characterization
Referral to oncologic specialist
Refer to gastrointestinal specialty guidelines
Select the morphology of the polyp:
Impression:
- Round up polyp size to the nearest millimeter.
- On follow-up:
- Increase of ≥ 4 mm in < 12 months OR reaches threshold size within category - recommend surgical consult
- Decrease of ≥ 4 mm - stop following
- Surgical consult may be an acceptable alternative for polyps 10-14 mm in Extremely Low Risk category
- It is optional to consider polyps Low Risk instead of Extremely Low Risk if certain ethnicities are known (North Indian, North/South American Indigenous, local incidence).
- If unsure between categories, choose Low Risk category.

Key facts for practice
Gallbladder polyps are found in roughly 5% of adults, and almost all of them are cholesterol or inflammatory pseudopolyps with no malignant potential. The 2022 Society of Radiologists in Ultrasound (SRU) consensus stratifies them by morphology first, size second: pedunculated ball-on-the-wall or thin-stalked polyps are extremely low risk, sessile or thick-stalked polyps are low risk, and any polyp with adjacent focal wall thickening of 4 mm or more is indeterminate risk. Most polyps 9 mm or smaller need no follow-up at all. Growth of 4 mm or more within 12 months, or reaching the size threshold for the category, triggers surgical consultation.[1]
SRU 2022 risk categories and follow-up intervals
The three categories are defined by morphology alone. Size then determines whether the polyp is ignored, followed, or referred.[1]
| Category | Morphology | Size | Recommendation |
|---|---|---|---|
| Extremely low risk | Pedunculated, "ball-on-the-wall" or thin stalk | ≤ 9 mm | No follow-up |
| Extremely low risk | Pedunculated, "ball-on-the-wall" or thin stalk | 10–14 mm | US at 6, 12 and 24 months (surgical consult is an acceptable alternative) |
| Extremely low risk | Pedunculated, "ball-on-the-wall" or thin stalk | ≥ 15 mm | Surgical consultation |
| Low risk | Sessile, or pedunculated with a thick or wide stalk | ≤ 6 mm | No follow-up |
| Low risk | Sessile, or pedunculated with a thick or wide stalk | 7–9 mm | US at 12 months |
| Low risk | Sessile, or pedunculated with a thick or wide stalk | 10–14 mm | US at 6, 12, 24 and 36 months, or surgical consultation |
| Low risk | Sessile, or pedunculated with a thick or wide stalk | ≥ 15 mm | Surgical consultation |
| Indeterminate risk | Adjacent focal gallbladder wall thickening ≥ 4 mm | ≤ 6 mm | US at 6, 12, 24 and 36 months, or surgical consultation |
| Indeterminate risk | Adjacent focal gallbladder wall thickening ≥ 4 mm | ≥ 7 mm | Surgical consultation |
Two rules apply across every category at follow-up: an increase of 4 mm or more within 12 months, or reaching the threshold size for that category, prompts surgical consultation; a decrease of 4 mm or more means follow-up can stop.[1] Note the asymmetry that catches people out — surveillance never runs beyond 3 years, and no category asks for indefinite annual scans.
Getting the morphology right
Because morphology drives the category, the scan itself matters more than the caliper. Four practical points:
- A thin stalk may be invisible on grayscale. It can be inferred from a polyp that wiggles in place, or demonstrated with color or power Doppler, microflow imaging, or contrast-enhanced US. Calling a thin-stalked polyp "sessile" because you could not see the stalk moves it from a no-follow-up category into a surveillance category unnecessarily.[1]
- Ball-on-the-wall means exactly that — a round polyp resting on a flat wall, like a ball on a table. It is extremely low risk.
- Sessile is flat or dome-shaped with a broad base and no stalk. Sessile morphology alone is enough to make a polyp low rather than extremely low risk.
- Look at the wall next to the polyp, not just the polyp. Focal wall thickening of 4 mm or more adjacent to the lesion is what defines the indeterminate risk category, and it is the feature most associated with malignancy.
If the study is technically inadequate — a poorly distended gallbladder, suboptimal technique, or a polyp that is not well seen — the SRU recommends a short-interval repeat ultrasound at 1–2 months with optimised preparation rather than assigning a category to a bad image. The same applies when tumefactive sludge or adenomyomatosis cannot be excluded, where CEUS or MRI may be used to characterise the lesion.[1] Both routes are built into the tool above.
Mimics that should not enter the algorithm
The SRU pathway applies to a lesion you are confident is a polyp. Several entities look polypoid and generate needless surveillance if they are categorised as polyps:
- Tumefactive sludge — mobile with position change, no internal vascularity, and often changes shape between images. Sludge larger than 10 mm that cannot be distinguished from a polyp is an explicit indication for short-interval repeat imaging or CEUS.
- Adenomyomatosis — intramural echogenic foci with comet-tail (twinkle) artifact from Rokitansky-Aschoff sinuses, and the "pearl necklace" sign on T2-weighted MRI. Focal fundal adenomyomatosis is the form most often mistaken for a sessile polyp with wall thickening.
- Adherent stones — non-shadowing small stones stuck to the wall can mimic polyps; roll the patient.
SRU versus the European (JES) guidelines
The most common source of confusion in reporting is that two major guidelines coexist and disagree. The 2022 Joint European Societies (JES) guidelines — ESGAR, EAES, EFISDS and ESGE — are size-and-risk-factor based rather than morphology based.[2]
| SRU 2022[1] | Joint European Societies 2022[2] | |
|---|---|---|
| Primary stratifier | Polyp morphology, then size | Polyp size, then patient risk factors |
| Surgery threshold | ≥ 15 mm (or ≥ 7 mm if indeterminate risk) | ≥ 10 mm |
| Risk factors | Not used for the core algorithm; geographic and genetic risk handled as a modifier | Age > 60 years, primary sclerosing cholangitis, Asian ethnicity, sessile lesion including focal wall thickening > 4 mm |
| 6–9 mm polyp | No follow-up if extremely low risk; 12-month US if low risk | Cholecystectomy if any risk factor present; otherwise US at 6 months, 1 year, 2 years |
| Growth trigger | ≥ 4 mm in 12 months, or reaching category threshold | Growth to 10 mm, or ≥ 2 mm within the 2-year follow-up period considered alongside risk factors |
| Follow-up duration | Maximum 3 years | Discontinue after 2 years if no growth |
The practical consequences have now been measured. In 135 resected polyps of 7 mm or larger, SRU had a sensitivity of 62% and specificity of 90% for neoplastic polyps, against JES sensitivity of 90% and specificity of 41% — SRU is the more specific instrument, JES the more sensitive one, and the difference in both directions was statistically significant.[3] Applied to consecutive patients, the SRU guidelines reduced follow-up imaging and surgical consultation costs by about 96% relative to the European guidelines,[4] and in a surgical referral cohort 52.5% of patients would have gone to immediate surgery under European guidelines versus 16.9% under SRU, a saving of $1,837 per person.[5]
Neither is simply "right". SRU suits the low-incidence populations of North America and Western Europe; where gallbladder cancer incidence is high, the higher sensitivity of the European approach is easier to defend. Say which guideline you are applying in the report.
Scenarios the original consensus did not spell out
A 2024 review by members of the SRU committee addressed the situations that surfaced once the guidelines were in daily use.[6]
- Primary sclerosing cholangitis — do not use the SRU algorithm. Defer to gastroenterology guidelines; the risk profile is entirely different.
- High geographic or genetic risk (for example North Indian, Indigenous North and South American, and other high-incidence populations) — an extremely low risk polyp may be managed one tier up, as low risk.
- Shrinking polyps — a 10–14 mm extremely low risk polyp, or a 7–14 mm low risk polyp, that decreases by 4 mm or more needs no further follow-up.
- Multiple polyps — multiplicity does not raise cancer risk. Categorise by the dominant polyp's morphology and size, not by the count.
- Vascular polyps — detectable flow does not raise cancer risk either, and does not change the category. Doppler is a tool for finding the stalk, not for risk-stratifying.
- Sessile polyps with features suggestive of cancer — these go straight to specialist referral rather than into the size table.
What the data since 2022 have shown
Three findings are worth carrying into practice.
Most polyps disappear from the pathway immediately. In 251 patients with 407 polyps, 51.6% were extremely low risk and 48.2% low risk, 96.3% were under 10 mm, and 88.4% required no follow-up at all under SRU. Of those followed, 89.6% were unchanged, smaller, or no longer visible. Of 28 patients who went on to cholecystectomy, 20 had no polyp found at pathology.[7]
Revised guidelines have not, by themselves, stopped unnecessary surgery. The Dutch POLYP study followed 302 patients across 26 centres; 88 underwent cholecystectomy, and of the 71 operated with a guideline-valid indication, 69% had non-neoplastic polyps and 32% had no gallbladder wall abnormality at all. Only six had an adenoma. Moving from the 2017 to the 2022 European guidelines changed the indication in only a handful of patients — solely through the age cut-off shifting from 50 to 60.[8] A guideline only helps if the report actually applies it.
Adherence is the bottleneck, and it is a reporting problem. Recommendations in gallbladder polyp reports are inconsistent enough that work is now being done on tooling — including large language model-based prompts — to embed SRU recommendations into the report at the point of dictation.[9] That is the gap the calculator on this page is meant to fill.
Reporting the finding
A usable impression names the size, the morphology, the resulting category, and the interval — the referring clinician should not have to open the guideline. For example:
8 mm pedunculated gallbladder polyp with a thin stalk, extremely low risk by SRU 2022 criteria. No imaging follow-up is recommended.
11 mm sessile gallbladder polyp, low risk by SRU 2022 criteria. Follow-up ultrasound at 6, 12, 24 and 36 months, or surgical consultation, is recommended. Surgical consultation should be obtained if the polyp increases by 4 mm or more within 12 months or reaches 15 mm.
The tool at the top of this page generates these impressions and copies them to the clipboard. For other incidental findings, the Fleischner calculator for pulmonary nodules and the full set of radiology calculators work the same way.
Frequently asked questions
Do all gallbladder polyps need follow-up?
No. Under the SRU 2022 guidelines, pedunculated ball-on-the-wall or thin-stalked polyps of 9 mm or smaller and sessile or thick-stalked polyps of 6 mm or smaller need no imaging follow-up whatsoever. In a real-world audit that accounted for 88% of all polyps detected.[7]
When does a gallbladder polyp need surgical referral?
At 15 mm or larger in the extremely low and low risk categories, at 7 mm or larger in the indeterminate risk category, or at any size if the polyp grows by 4 mm or more within 12 months or reaches its category threshold. Under the European guidelines the threshold is 10 mm, or 6–9 mm with a malignancy risk factor.[1][2]
How long should gallbladder polyps be followed?
Three years at most under SRU, and two years under the European guidelines. Neither supports indefinite surveillance of a stable small polyp. If the polyp shrinks by 4 mm or more, or is no longer seen, stop.[1][2]
What does focal wall thickening next to a polyp mean?
Adjacent focal wall thickening of 4 mm or more places the polyp in the indeterminate risk category regardless of its size, because it raises concern for an underlying mass. If the polyp component is 7 mm or larger, refer for surgical consultation rather than scheduling follow-up.[1]
Do multiple gallbladder polyps carry a higher cancer risk?
No. Neither the number of polyps nor demonstrable vascularity within a polyp increases the risk of gallbladder cancer. Categorise on morphology and size alone.[6]
Which guideline should I use, SRU or European?
Follow your department's policy and state it in the report. SRU is more specific and generates far fewer follow-up scans and operations; the European guidelines are more sensitive and are easier to justify where gallbladder cancer incidence is high.[3][4][5]
Watch Aya Kamaya's SRU consensus presentation for the reasoning behind the categories:

Disclaimer: This tool is educational, is not a substitute for clinical judgment, and is not affiliated with or verified by the SRU.
References
- Kamaya A, Fung C, Szpakowski JL, et al. Management of Incidentally Detected Gallbladder Polyps: Society of Radiologists in Ultrasound Consensus Conference Recommendations. Radiology. 2022;305(2):277–289. PMID: 35787200. doi:10.1148/radiol.213079
- Foley KG, Lahaye MJ, Thoeni RF, et al. Management and follow-up of gallbladder polyps: updated joint guidelines between the ESGAR, EAES, EFISDS and ESGE. Eur Radiol. 2022;32(5):3358–3368. PMID: 34918177. doi:10.1007/s00330-021-08384-w
- Nanda BP, Moloney BM, Gershon A, et al. Resected gallbladder polyps: comparison of the 2022 Society of Radiologists in Ultrasound and Joint European Societies Guidelines' diagnostic performance. Eur Radiol. 2026;36(1):462–472. PMID: 40711552. doi:10.1007/s00330-025-11826-4
- Vo-Phamhi JM, Tiyarattanachai T, Matuszczak M, et al. Follow-up Imaging and Surgical Costs Associated with Different Guidelines for Management of Incidentally Detected Gallbladder Polyps. Acad Radiol. 2025;32(2):757–766. PMID: 38862347. doi:10.1016/j.acra.2024.05.034
- Garcia L, Dygean F, Bortree E, et al. A comparison of society guidelines in the management of gallbladder polyps. Am J Surg. 2025;240:116099. PMID: 39571191. doi:10.1016/j.amjsurg.2024.116099
- Knight J, Kamaya A, Fetzer D, et al. Management of incidentally detected gallbladder polyps: a review of clinical scenarios using the 2022 SRU gallbladder polyp consensus guidelines. Abdom Radiol (NY). 2024;49(9):3158–3165. PMID: 38411693. doi:10.1007/s00261-024-04197-9
- Jeans M, Dragh M, Necas M. Size and Morphology of Ultrasound Detected Gallbladder Polyps and the Surveillance Implications of Adopting the Society of Radiologists in Ultrasound Consensus Conference Recommendations: A Waikato Experience. J Med Imaging Radiat Oncol. 2025;69(3):335–341. PMID: 40146883. doi:10.1111/1754-9485.13854
- van Dooren M, de Savornin Lohman EAJ, van der Bilt J, et al. Revised Guidelines for the Treatment and Follow-Up of Gallbladder Polyps Do Not Reduce Unwarranted Cholecystectomies: Results of the POLYP Study. United European Gastroenterol J. 2025;13(7):1133–1140. PMID: 40697033. doi:10.1002/ueg2.70057
- Mugu VK, Carr BM, Olson MC, et al. Increasing Adherence to Societal Recommendations in Radiology Reporting: A Feasibility Study Using Society of Radiologists in Ultrasound Guidelines for Incidentally Detected Gallbladder Polyps. Ultrasound Q. 2024;41(1):e00699. PMID: 39690147. doi:10.1097/RUQ.0000000000000699

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
About the Author
Dr. Amar Udare, MD, DNB
Dr. Udare holds an MBBS and MD degree, and his expertise lies in the field of radiology. He has authored multiple peer-reviewed publications, contributing significantly to the medical field. His works can be accessed on PubMed and Google Scholar.
In addition to his academic and professional achievements, Dr. Udare is an avid reader and enjoys exploring the latest advancements in medical technology. His commitment to making complex medical knowledge accessible to patients and the general public aligns with our mission at RadioGyan.com.
For any further questions or clarifications, feel free to reach out to Dr. Udare via the contact form.