
42 yr male with a history of neonatal umbilical vein catheterization presenting with hematemesis and splenomegaly.
Diagnosis and teaching points:
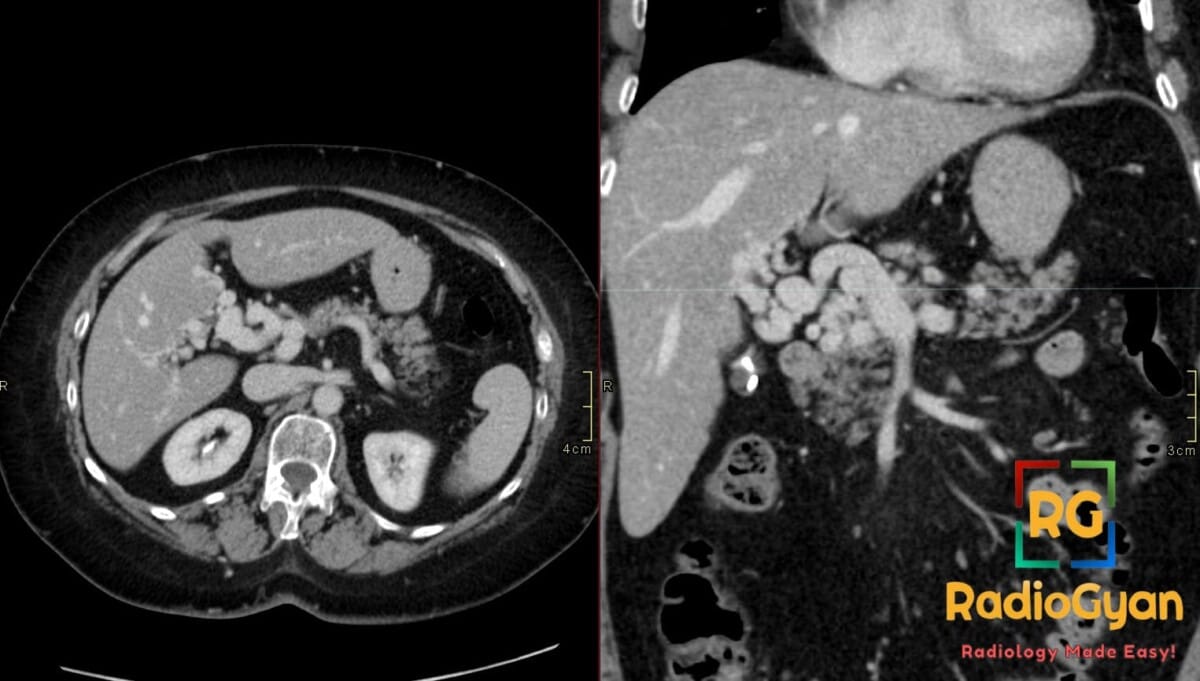
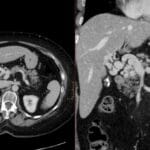
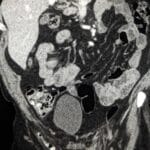
Diagnosis: Cavernous transformation of the portal vein
Key facts for boards exams:
• Cavernous transformation represents the chronic sequela of portal vein thrombosis (PVT) where a “cavernoma” of tortuous collateral vessels develops to bypass an obliterated portal vein.
• The most common clinical presentation involves sequelae of portal hypertension, such as variceal bleeding, splenomegaly, and ascites.
• Portal cavernoma cholangiopathy may occur when periportal collaterals compress the bile ducts, potentially seen on MRCP as peribiliary stenoses.
- Clinical: Occurs in any age or sex; symptoms include variceal bleeding, ascites, splenomegaly, and hypersplenism; risk factors include prior PVT from hypercoagulable states, neonatal umbilical vein catheterization, or abdominal sepsis.
- Etiology/Pathophys: Chronic sequela of portal vein thrombosis where neovascularization forms multiple small portoportal and portosystemic collaterals in the porta hepatis.
- US: Anechoic tortuous collaterals or a sponge-like mass in the porta hepatis; color Doppler shows a serpiginous mixed-color pattern with hepatopetal flow and absent flow in the native portal vein.
- CT: Nonvisualization of the main portal vein trunk replaced by numerous tortuous periportal collaterals (cavernoma); may appear as a solid tumor-like enhancing hilar mass; associated signs include splenomegaly and gallbladder varices.
- MRI: Tortuous peri-hilar vessels replacing the native portal vein; MRCP may show peribiliary stenoses from extrinsic compression by collaterals (portal cavernoma cholangiopathy).
- Signs: Portal cavernoma: A sponge-like mass or tangle of enhancing vessels in the porta hepatis representing dilated periportal collaterals.
- Frameworks: Described by extent (extrahepatic vs. intrahepatic) and chronicity; portal vein mapping is critical prior to liver transplantation.
- DDx: Tumor thrombus (shows arterial enhancement and contiguous primary tumor); Lymphadenopathy (solid and non-vascular on Doppler); Acute PVT (echogenic thrombus without the presence of collateral cavernoma).
- Tx: Management of underlying portal hypertension (beta-blockers, TIPS, endoscopic variceal band ligation) and anticoagulation for the initial thrombosis.
OSCE Questions
Question: What is the most characteristic finding of this condition on cross-sectional imaging of the porta hepatis?
A sponge-like mass of multiple tortuous, enhancing periportal collateral vessels replacing the native portal vein.
Question: What is the underlying pathophysiology that leads to the development of this condition?
It is a chronic sequela of portal vein thrombosis where the original lumen obliterates and is replaced by portoportal neovascularization.
Question: How can this condition be distinguished from malignant tumor thrombus on contrast-enhanced CT or MRI?
Malignant thrombus typically demonstrates internal arterial phase enhancement, while this condition features a network of periportal collaterals bypassing a bland obstruction.
Question: What secondary complication may be visualized on MRCP as a result of these vascular changes?
Portal cavernoma cholangiopathy, characterized by peribiliary stenoses or indentations from the adjacent collateral vessels.
Question: What are the expected flow characteristics of the substituted vessels when evaluated with Color Doppler Ultrasound?
A serpiginous mixed-color pattern representing hepatopetal flow with a loss of normal portal phasicity.
MCQ Questions
1. What is the primary etiology of this vascular pathology?
A. Congenital venous malformation
B. Chronic portal vein thrombosis
C. Acute pyogenic pylephlebitis
D. Hepatic artery aneurysm
Answer: B. Chronic portal vein thrombosis. This condition represents the chronic sequela of portal vein thrombosis where collaterals replace the primary vessel.
2. Which imaging finding is most characteristic of this condition?
A. Solitary hilar soft tissue mass
B. Large caliber main portal vein
C. Tangle of tortuous periportal vessels
D. Gas within the portal system
Answer: C. Tangle of tortuous periportal vessels. These “cavernoma” collaterals form a sponge-like mass to bypass the obliterated native portal vein.
3. What direction of flow is typically seen in these collaterals on Doppler?
A. Hepatopetal
B. Hepatofugal
C. Bidirectional (To-and-Fro)
D. Absent flow
Answer: A. Hepatopetal. Despite the native vein being thrombosed, the periportal collaterals carry blood toward the liver.
4. Which associated biliary finding may be seen on MRCP?
A. Intraluminal stones
B. Choledochal cyst
C. Common bile duct agenesis
D. Extrinsic compression by collaterals
Answer: D. Extrinsic compression by collaterals. Portal cavernoma cholangiopathy occurs when venous collaterals cause stenoses of the bile ducts.
5. How is this pathology differentiated from malignant tumor thrombus?
A. Presence of splenomegaly
B. Vessel diameter over 2cm
C. Lack of internal arterial enhancement
D. Presence of ascites
Answer: C. Lack of internal arterial enhancement. Unlike bland thrombus and its collaterals, malignant thrombus typically demonstrates internal neo-vascularity and arterial enhancement.
Check out more such cases:




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case