
25-year-old male presenting with acute left scrotal pain and swelling. What is your diagnosis?
Diagnosis and teaching points:
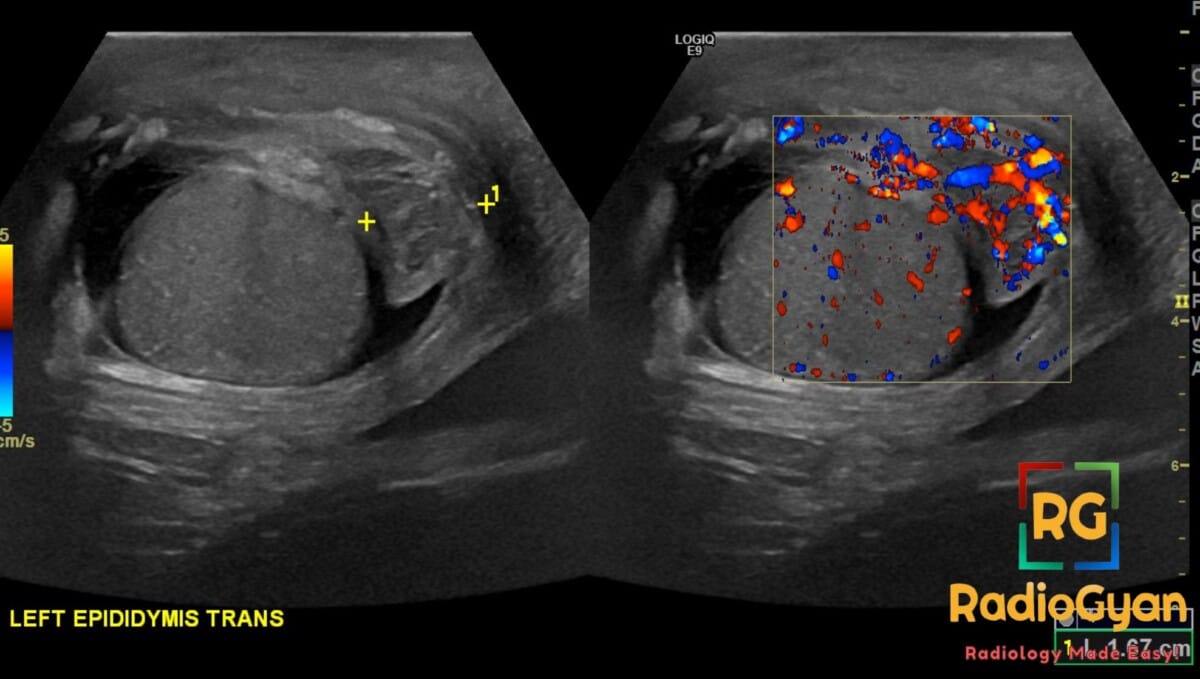
Diagnosis: Left epididymo-orchitis.
Key facts for board exams:
- Most common cause of acute scrotum in post-pubertal and adult males; testicular torsion is the primary differential in adolescents.
- Scrotal ultrasound with color Doppler hyperemia (increased blood flow) is the hallmark finding and the key feature distinguishing it from torsion.
- Most cases result from ascending infection from the urinary tract (urethra/prostate).
- In men <35 years, consider Chlamydia trachomatis and Neisseria gonorrhoeae; in men >35 years or with BPH/urinary stasis, consider E. coli and other gram-negative organisms.
- Cremasteric reflex is preserved (absent in torsion); positive Prehn sign (pain relief with scrotal elevation).
Detailed teaching points:
- Clinical: Presents with unilateral scrotal pain, swelling, erythema, and fever; may have dysuria or urinary symptoms; common in sexually active young men and older men with BPH, strictures, or recent instrumentation.
- Etiology/Pathophys: Bacterial infection reaches the epididymis via retrograde ascent through the vas deferens, often spreading contiguously to involve the testis (epididymo-orchitis).
- Radiograph: Not applicable for scrotal pathology.
- US: Enlarged epididymis (most commonly the tail) and/or testis; increased color and spectral Doppler flow (hyperemia); reactive hydrocele; thickened scrotal wall; heterogeneous echotexture; complex/epididymal abscess may appear as a focal hypoechoic or anechoic area with debris.
- CT: Usually not required; may show scrotal wall thickening, fat stranding, and an enlarged enhancing epididymis/testis when imaged for other indications.
- MRI: Not first-line; T2 hyperintense enlarged epididymis/testis with avid post-contrast enhancement if performed.
- Nuc Med: Not routinely used; testicular scintigraphy would show increased perfusion and delayed uptake (vs. cold spot in torsion).
- Signs: Color Doppler hyperemia (increased intratesticular/epididymal flow) is the cardinal sign; preserved cremasteric reflex clinically; complex hydrocele with internal echoes is a supportive feature.
- Frameworks: No formal staging system; severity graded sonographically as focal vs. diffuse epididymitis, epididymo-orchitis, or complicated (abscess/infarction/necrosis).
- DDx: Testicular torsion (decreased/absent Doppler flow, absent cremasteric reflex, younger age, <6h window for salvage); torsion of the appendix testis (normal testicular flow, palpable blue-dot sign, small avascular nodule near upper pole); testicular tumor (focal solid mass, often with internal vascularity but lacking diffuse hyperemia and inflammatory features); fournier gangrene (subcutaneous gas, severe systemic toxicity, surgical emergency).
- Tx: Empirical antibiotics (ceftriaxone + doxycycline for STI coverage in <35; fluoroquinolone for enteric organisms in >35), scrotal support, analgesia, and follow-up ultrasound to exclude underlying tumor or abscess; urology referral if torsion cannot be excluded or if abscess/necrotizing infection is suspected.
OSCE Questions
Question: What is the first-line imaging modality for evaluating this condition?
Scrotal ultrasound with color Doppler.
Question: What is the most critical diagnosis to exclude using color Doppler?
Testicular torsion — demonstrated by absent or decreased intratesticular blood flow.
Question: What is the most common bacterial cause in sexually active men under 35?
*Chlamydia trachomatis* (with *Neisseria gonorrhoeae* being the other primary STI cause).
Question: What viral pathogen classically causes bilateral involvement of this condition?
Mumps virus.
Question: What complication requires surgical drainage in this condition?
Scrotal abscess.
MCQ Questions
1. Which epididymal region is classically affected first?
A. Tail
B. Head
C. Body
D. Vas deferens
Answer: A. Tail. Inflammation spreads contiguously from the tail toward the head and adjacent testis.
2. Which Doppler finding most reliably excludes testicular torsion?
A. Increased resistive index
B. Absent venous flow
C. Marked hyperemia
D. Reversed diastolic flow
Answer: C. Marked hyperemia. Preserved or increased arterial flow excludes complete spermatic cord torsion.
3. In sexually active young men, this entity is most commonly caused by:
A. E. coli and Proteus
B. Chlamydia and Gonorrhea
C. Mumps and coxsackie
D. Staph and Strep
Answer: B. Chlamydia and Gonorrhea. STI pathogens predominate in sexually active men under 35.
4. Which finding is characteristic of the emphysematous variant?
A. Calcified scrotal plaque
B. Fat-fluid level
C. Scrotal wall thickening
D. Intrascrotal gas
Answer: D. Intrascrotal gas. Gas-forming organisms produce parenchymal gas, best detected on CT.
5. Which risk factor most commonly predisposes older men?
A. Bladder outlet obstruction
B. Varicocele
C. Vasectomy
D. Cryptorchidism
Answer: A. Bladder outlet obstruction. Urinary stasis permits retrograde ascent of enteric bacteria into the ejaculatory ducts. [/spoiler
Check out more such cases:



Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case