
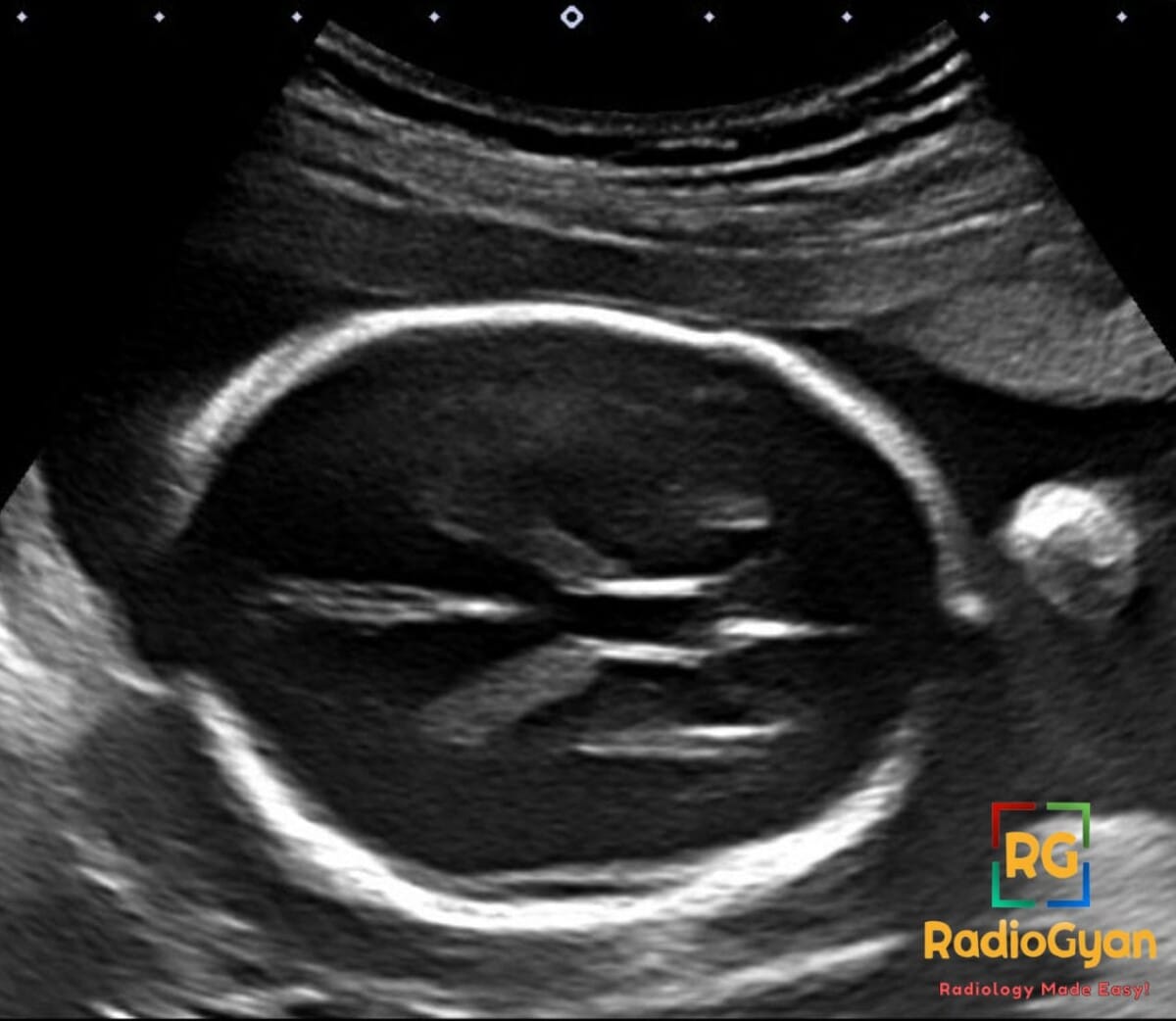
Routine fetal anomaly ultrasound in a 22-week pregnancy.
Diagnosis and teaching points:
Diagnosis: Cavum vergae normal variant
Key facts for boards exams:
- Cavum vergae is a normal anatomical variant representing the posterior extension of the cavum septi pellucidi, located posterior to the forniceal columns.
- It is an extra-pial, CSF-filled space that does not communicate with the ventricular system or the subarachnoid space.
- The structure typically obliterates in a caudal-to-rostral direction, usually closing by 3-6 months postnatally.
- On fetal ultrasound specifically between 18-37 weeks, visualize of the cavum septi pellucidi (and often the vergae) is a mandatory landmark for normal brain development.
- It is considered an incidental, asymptomatic finding in the vast majority of cases and requires no treatment.
Detailed teaching points:
- Clinical: Present in 100% of 6-month-old fetuses and ~30% of term infants; persists in <2% of adults; typically asymptomatic.
- Etiology/Pathophys: Results from incomplete fusion of the septal leaflets posterior to the forniceal columns; it is not a true cyst as it lacks an epithelial lining.
- US: Appears as a midline anechoic cystic structure posterior to the foramen of Monro, situated beneath the splenium of the corpus callosum and above the fornices.
- CT: Midline CSF-density (0-10 HU) space with thin walls (<2 mm); shows no enhancement or surrounding edema.
- MRI: Follows CSF signal on all sequences (T1 hypointense, T2 hyperintense, FLAIR suppressed); sagittal views best demonstrate its position posterior to the fornix columns.
- Signs: Double cavum refers to the simultaneous presence of the cavum septi pellucidi and the cavum vergae separated by the vertical plane of the fornices.
- Frameworks: Evaluated primarily by size on fetal scans; presence after 37 weeks or in adulthood is noted as a variant.
- DDx: Cavum velum interpositum (located below the fornices, superior to pineal, communicates with subarachnoid space); Arachnoid cyst (shows mass effect and internal communication).
- Tx: Standard management is observation and reassurance as it is a benign normal variant.
OSCE Questions
Question: Anatomically, what structures form the superior and posterior boundaries of this pathology?
The corpus callosum body forms the superior boundary and the splenium forms the posterior boundary.
Question: By what gestational age is this condition expected to be present in nearly all fetuses?
This condition is present in 100% of fetuses by 6 months (approximately 24-28 weeks) gestation.
Question: How is this condition distinguished from a cavum velum interpositum on sagittal imaging?
This condition is located above the fornix, whereas the cavum velum interpositum is located below the fornix.
Question: What is the primary developmental mechanism responsible for the appearance of this condition?
Incomplete posterior-to-anterior fusion of the laminae of the septum pellucidum.
Question: What midline structure serves as the landmark to differentiate this pathology from a cavum septi pellucidi?
The columns of the fornix serve as the anatomical dividing line between the two spaces.
MCQ Questions
1. Where is this anatomical variant located relative to the columns of the fornix?
A. Anterior
B. Lateral
C. Posterior
D. Superior
Answer: C. Posterior. This variant represents the posterior extension of the cavum septi pellucidi, located behind the forniceal columns.
2. Which structure forms the superior border of this fluid-filled space?
A. Optic chiasm
B. Corpus callosum
C. Third ventricle
D. Pons
Answer: B. Corpus callosum. The body and splenium of the corpus callosum form the superior boundary of this space.
3. How does this variant typically change in the first months of postnatal life?
A. Expands rapidly
B. Calcifies
C. Involutes and fuses
D. Develops enhancement
Answer: C. Involutes and fuses. This embryonic space typically undergoes caudocranial fusion, closing in about 98% of adults.
4. Which feature distinguishes this variant from a cavum velum interpositum?
A. CSF signal intensity
B. Midline location
C. Communication with subarachnoid space
D. Absence of mass effect
Answer: C. Communication with subarachnoid space. Unlike this variant, the cavum velum interpositum communicates with the subarachnoid space and lacks septal leaflets.
5. What is the standard management for this finding on a fetal ultrasound?
A. Immediate neurosurgical consult
B. Termination of pregnancy
C. Intrauterine shunting
D. Reassurance as a normal variant
Answer: D. Reassurance as a normal variant. This is a benign anatomical variant that usually requires no intervention or follow-up.
Check out more such cases:




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case