
- Key facts for practice and radiology exams
- The six Schatzker types at a glance
- Characteristics of the individual types
- Why CT changed how the classification is used
- The updated (2018) CT-based Schatzker classification
- Associated soft-tissue and neurovascular injuries
- Reporting checklist
- Case example
- Frequently asked questions
- References and further reading
Key facts for practice and radiology exams
The Schatzker classification sorts tibial plateau fractures into six types of increasing severity. The single most useful split is low-energy (types I–III), which involve only the lateral plateau, versus high-energy (types IV–VI), which involve the medial plateau or both condyles and carry a far higher rate of neurovascular and soft-tissue injury. It was first described on radiographs, but CT is now the standard tool for assessment and routinely upgrades the type and changes the surgical plan. In 2018 Kfuri and Schatzker themselves revised the system to a CT-based, three-dimensional version that adds anterior/posterior column modifiers, because the original two-dimensional scheme under-recognises posterior fragments.[1][2][3]
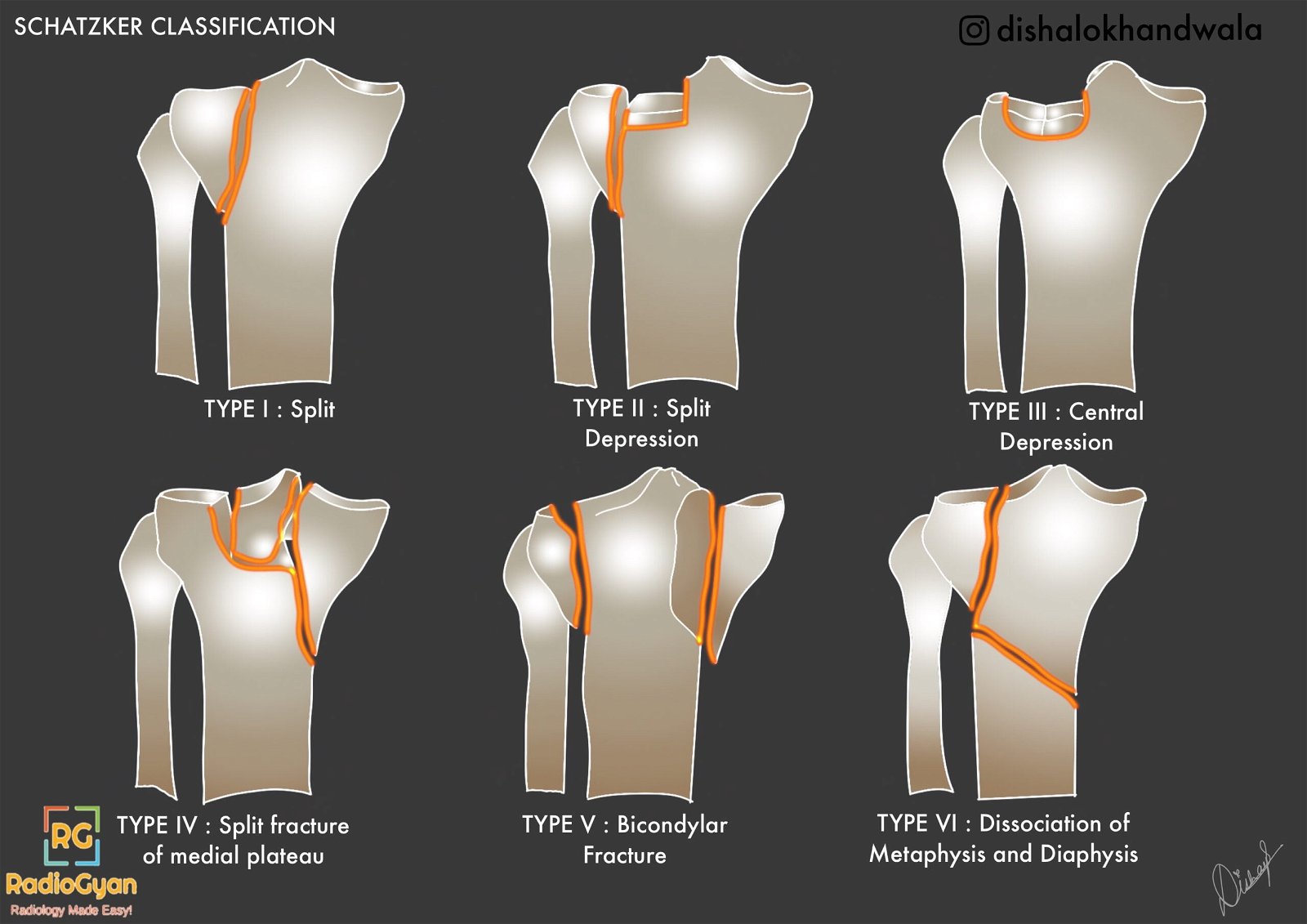
The six Schatzker types at a glance
Type I — Lateral plateau split (cleavage), no or minimal (<4 mm) depression
Type II — Lateral plateau split with depression
Type III — Pure lateral plateau depression (IIIA lateral, IIIB central)
Type IV — Medial plateau fracture
Type V — Bicondylar fracture (both plateaus)
Type VI — Plateau fracture with metaphyseal–diaphyseal dissociation
Types I–III are low-energy injuries; types IV–VI are high-energy injuries.
The lateral plateau is involved in the majority of tibial plateau fractures (roughly 55–70%), which is why the low-energy lateral types (I–III) together are the most common presentation. The percentages below are approximate and vary between series.[2]
Characteristics of the individual types
| Type | Characteristics |
|---|---|
| I | – Wedge-shaped pure cleavage (split) fracture of the lateral tibial plateau. – Approximately 6% of tibial plateau fractures. – More frequent in younger patients with normal bone mineralisation. – May be subtle on radiographs and confused with a type II fracture. – Can be associated with a distraction-type MCL or ACL injury. – Treatment: open reduction and internal fixation, with or without arthroscopy. |
| II | – Combined cleavage and compression: a type I split with an added depressed component of the lateral plateau. – Depression can be difficult to appreciate on plain radiographs. – Depression is measured as the vertical distance between the lowest point of the intact medial plateau and the lowest depressed lateral fragment. – Approximately 25% of tibial plateau fractures; common in the 4th decade. – Associated distraction injury of the MCL or medial meniscus. – Treatment: open reduction, elevation of the depressed fragment, bone grafting and buttress fixation. |
| III | – Pure compression (depression) fracture of the lateral (IIIA) or central (IIIB) plateau, with the articular surface driven into the metaphysis by axial load. – Approximately a third of cases in some series; common in the 4th–5th decade and in osteoporotic bone. – Treatment: IIIA may be non-operative; IIIB is usually elevated through a metaphyseal cortical window, grafted and buttressed. |
| IV | – Medial plateau fracture (split, depressed, or both). Approximately 10% of cases. – High-energy fracture-dislocation pattern with a poorer prognosis. – High risk of injury to the peroneal nerve, popliteal vessels and the posterolateral corner / lateral collateral ligament. – Treatment: open reduction and internal fixation; assess and document neurovascular status. |
| V | – Bicondylar fracture involving both plateaus, classically with an inverted-Y appearance. – High-energy injury; ACL and meniscal involvement common. The metaphysis remains in continuity with the diaphysis. – Often managed initially with spanning external fixation to let soft-tissue swelling settle before definitive fixation. |
| VI | – Plateau fracture with metaphyseal–diaphyseal dissociation (the joint surface is separated from the shaft). – Approximately 20% of cases; highest-energy pattern. – Associated with extensive soft-tissue injury and the highest risk of compartment syndrome — assess compartments explicitly. |
Why CT changed how the classification is used
The Schatzker types were defined on plain radiographs, but two-dimensional imaging systematically under-reads these injuries. CT with multiplanar reformats and 3D reconstruction more accurately measures the depth of articular depression, detects occult split lines, and identifies posterior fragments that a frontal radiograph hides. Multiple studies have shown that surgical plans based on radiographs are revised after CT — the Schatzker type is frequently upgraded, most often to a higher, higher-energy type. MRI adds assessment of the menisci, cruciate and collateral ligaments, which are injured in a large proportion of these fractures.[2]
Practical consequence: a CT (with reformats) should be obtained for essentially every tibial plateau fracture being considered for surgery, and the report should state the true depth of depression, the number and location of fragments, and the degree of comminution — not just the Schatzker number.
The updated (2018) CT-based Schatzker classification
More than four decades after the original description, Kfuri and Schatzker published a revised, three-dimensional version of the classification built for the CT era.[1] It keeps the familiar six-type template but adds spatial detail that determines the surgical approach and patient positioning:
- Two columns. The tibial plateau is divided into a lateral and a medial column.
- A virtual equator. A line in the coronal plane splits each column into an anterior (A) and a posterior (P) quadrant.
- Location modifiers. Unicondylar types (I–IV) gain an A or P modifier to state where the main fracture plane sits. Bicondylar types (V and VI) carry A/P modifiers for each column, plus L (lateral) and M (medial) to name the column of the principal fragment.
- The main fracture plane. Recognising the exact location of the principal fracture plane guides patient positioning, choice of surgical approach, and where to place the buttress plate for stable fixation.
This dovetails with the three-column concept described by Luo et al., which splits the proximal tibia into lateral, medial and posterior columns on an axial CT image. A fragment isolated in the posterior column is the fracture most often missed by the classic Schatzker scheme, and it typically needs a dedicated posterior approach and buttress plate rather than a standard anterolateral one.[4] In a further 2022 update, Schatzker and Kfuri re-emphasised that joint stability — determined by the location of the split wedge fragment and the continuity of the articular rim — is what should drive the decision to operate.[5]
Associated soft-tissue and neurovascular injuries
Tibial plateau fractures are rarely isolated bony injuries. Meniscal tears, cruciate and collateral ligament injuries are common, and the higher-energy medial and bicondylar patterns carry specific vascular and nerve risks that must be looked for and documented.
| Pattern | Look specifically for |
|---|---|
| Lateral (types I–III) | Lateral meniscal tear, distraction injury of the MCL, ACL avulsion; a Segond fracture flags ACL injury. |
| Medial (type IV) | Popliteal artery and peroneal nerve injury, posterolateral corner and lateral collateral ligament disruption — this is a fracture-dislocation. |
| Bicondylar / dissociated (types V–VI) | Compartment syndrome (highest risk in type VI), extensive soft-tissue injury, vascular compromise; ACL and meniscal tears are common. |
Reporting checklist
A useful CT report of a tibial plateau fracture goes well beyond the Schatzker number:
- Schatzker type (and, where possible, the updated column/quadrant location — lateral vs medial, anterior vs posterior).
- Maximum articular depression in millimetres, and the condylar widening — both influence the decision to operate.
- Number and location of fragments, degree of comminution, and any separate posterior column fragment.
- Metaphyseal–diaphyseal extension (which makes it a type VI).
- Associated injuries — menisci, cruciate and collateral ligaments, and any sign of vascular injury or impending compartment syndrome.
Case example

The fracture above is a Schatzker type II tibial plateau fracture. Click here for more images.
Frequently asked questions
What is the Schatzker classification of tibial plateau fractures?
It is a system that divides tibial plateau fractures into six types (I–VI) of increasing severity. Types I–III involve the lateral plateau and are low-energy; types IV–VI involve the medial plateau or both condyles and are high-energy. It guides assessment, surgical planning and prognosis.
Which Schatzker types are low-energy and which are high-energy?
Types I, II and III are low-energy injuries confined to the lateral plateau. Types IV, V and VI are high-energy injuries involving the medial plateau or both condyles, with a much higher rate of neurovascular and soft-tissue injury.
What is the difference between a Schatzker type V and type VI fracture?
A type V is a bicondylar fracture involving both plateaus, but the joint surface stays in continuity with the tibial shaft. A type VI adds metaphyseal–diaphyseal dissociation — the articular block is separated from the shaft — and carries the highest risk of compartment syndrome.
Why is CT used to classify tibial plateau fractures?
Plain radiographs under-read these injuries. CT measures the true depth of articular depression, detects occult splits and posterior fragments, and frequently upgrades the Schatzker type and changes the surgical plan. MRI adds meniscal and ligament assessment.
Was the Schatzker classification updated?
Yes. In 2018 Kfuri and Schatzker published a CT-based, three-dimensional revision that keeps the six types but adds lateral/medial column and anterior/posterior quadrant modifiers to locate the main fracture plane. It addresses posterior fragments that the original two-dimensional scheme tended to miss.
References and further reading
- Kfuri M, Schatzker J. Revisiting the Schatzker classification of tibial plateau fractures. Injury. 2018;49(12):2252–2263. PMID: 30526924. doi:10.1016/j.injury.2018.11.010
- Markhardt BK, Gross JM, Monu JUV. Schatzker classification of tibial plateau fractures: use of CT and MR imaging improves assessment. RadioGraphics. 2009;29(2):585–597. PMID: 19325067. doi:10.1148/rg.292085078
- Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968–1975. Clin Orthop Relat Res. 1979;(138):94–104. PMID: 445923
- Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma. 2010;24(11):683–692. PMID: 20881634. doi:10.1097/BOT.0b013e3181d436f3
- Schatzker J, Kfuri M. Revisiting the management of tibial plateau fractures. Injury. 2022;53(6):2207–2218. PMID: 35491279. doi:10.1016/j.injury.2022.04.006
Illustration contributed by #TeamGyan member Dr. Disha Lokhandwala.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case