
| NASCET | ECST ≈ | Grade | Symptomatic management |
|---|---|---|---|
| < 50% | < 70% | Mild | Best medical therapy; no revascularization |
| 50–69% | 70–82% | Moderate | CEA reasonable in selected patients (greater benefit in men, early surgery) |
| 70–99% | 82–99% | Severe | CEA (or CAS) recommended, ideally within 2 weeks |
| Near-occlusion | Near-occlusion | Distal ICA collapsed | Individualized; revascularization benefit uncertain |
| 100% | 100% | Occlusion | Not amenable to revascularization |
| Category (NASCET) | ICA PSV | ICA/CCA ratio | ICA EDV |
|---|---|---|---|
| Normal | < 125 cm/s | < 2.0 | < 40 cm/s |
| < 50% | < 125 cm/s | < 2.0 | < 40 cm/s |
| 50–69% | 125–230 cm/s | 2.0–4.0 | 40–100 cm/s |
| ≥ 70% (< near-occl.) | > 230 cm/s | > 4.0 | > 100 cm/s |
| Near-occlusion | High, low or undetectable | Variable | Variable |
| Total occlusion | No flow | — | — |
This tool implements the NASCET and ECST measurement methods and the SRU Doppler consensus. Final grading and management must be made by a qualified physician using the full study, the clinical presentation (symptomatic vs asymptomatic) and your laboratory’s validated criteria.
NASCET / ECST Carotid Stenosis Calculator
This carotid stenosis calculator grades internal carotid artery (ICA) narrowing by the two reference methods used worldwide — the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method and the European Carotid Surgery Trial (ECST) method — and generates an editable, dictation-ready report. Enter the luminal diameters from CTA, MRA or catheter angiography, or enter the carotid Doppler ultrasound velocities, and the tool returns the stenosis percentage by each method, the equivalent value in the other method, the severity grade, and the corresponding management guidance for symptomatic and asymptomatic disease.
NASCET and ECST were the landmark randomised trials that defined when carotid endarterectomy reduces stroke. Crucially, they measured the same stenosis against different reference diameters, so a given lesion carries a higher percentage by ECST than by NASCET. Modern guidelines and ultrasound criteria are anchored to the NASCET method, but ECST values remain common in European practice and in older reports, which makes reliable conversion between the two essential. This calculator implements both, converts between them, and maps Doppler velocities onto the NASCET scale using the Society of Radiologists in Ultrasound (SRU) consensus.
NASCET vs ECST: How the Methods Differ
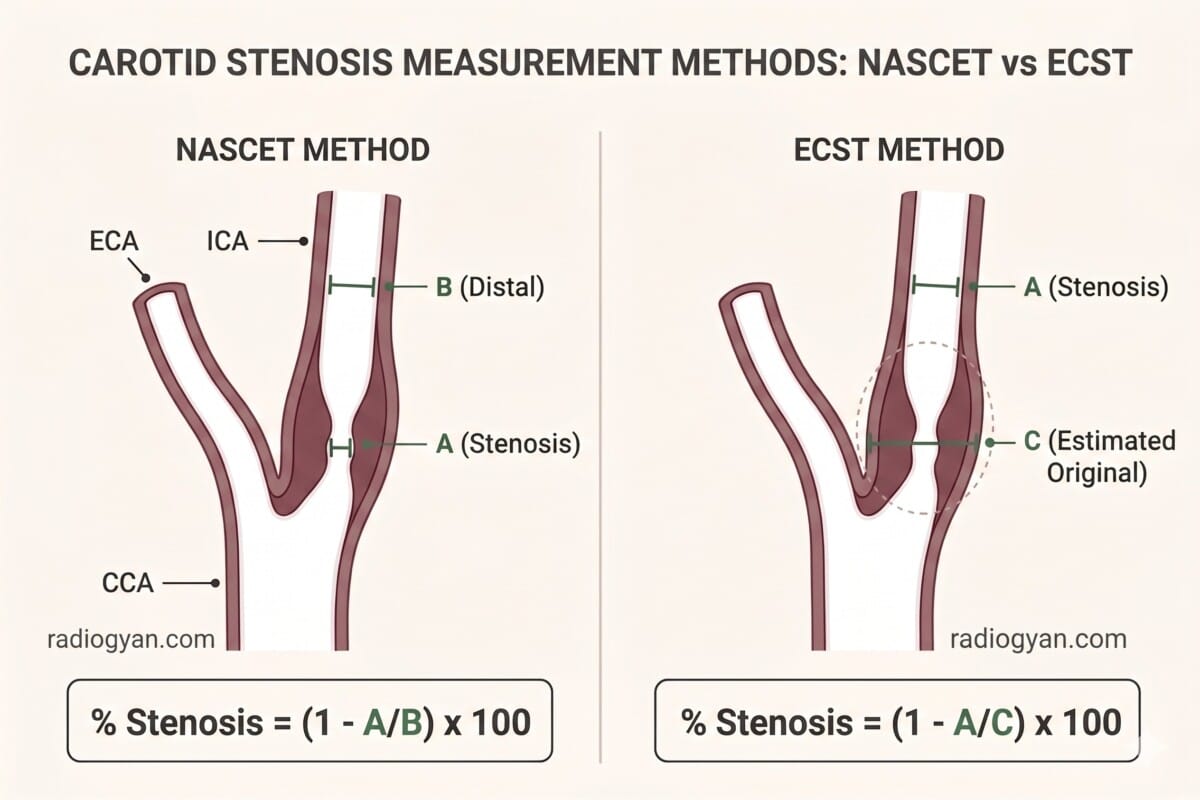
Both methods express stenosis as a percentage diameter reduction, but they use a different denominator:
- NASCET = (1 − A / B) × 100, where A is the narrowest residual lumen and B is the diameter of the normal internal carotid artery distal to the stenosis, at the point where the walls become parallel.
- ECST = (1 − A / C) × 100, where C is the estimated original diameter of the carotid bulb at the site of maximal stenosis.
Because the carotid bulb is wider than the distal ICA, the ECST denominator is larger and ECST therefore yields a higher percentage for the same lesion. The two scales are linked by a simple, widely cited equation derived by Rothwell and colleagues:
For example, a 70% NASCET stenosis corresponds to roughly 82% by ECST, and a 50% NASCET stenosis corresponds to about 70% ECST. The calculator applies this conversion automatically: enter just one reference diameter and it estimates the value in the other method, clearly labelling which figure was measured and which was converted.
When This Calculator Applies
Use it to grade extracranial internal carotid artery stenosis at the carotid bifurcation, whether measured directly on cross-sectional or catheter angiography or estimated from a carotid duplex study. The single most severe point of narrowing determines the grade. The tool does not apply to intracranial stenosis (which is graded by the WASID method), to common carotid or external carotid disease, or to in-stent restenosis, for which dedicated velocity criteria exist. Management recommendations depend heavily on whether the stenosis is symptomatic (ipsilateral TIA, ischaemic stroke or amaurosis fugax within the preceding six months) or asymptomatic, so select the clinical context before reading the recommendation.
How to Use the Carotid Stenosis Calculator
- Choose the clinical context – symptomatic or asymptomatic – so the management guidance reflects the correct revascularization threshold.
- Pick the input method. For diameter measurement, enter the narrowest residual lumen (A) plus the distal normal ICA (B, for NASCET) and/or the estimated original bulb diameter (C, for ECST). For Doppler ultrasound, enter the ICA peak systolic velocity (PSV) with the optional end-diastolic velocity (EDV) and common carotid PSV for the ratio.
- Flag near-occlusion or occlusion when the distal ICA is collapsed (string sign) or there is no detectable flow – the percentage formulae and velocity thresholds are unreliable in these states.
- Read and copy the result. The category, the NASCET and ECST percentages, and the management recommendation update automatically, and a copyable report block is generated for your reporting system.
Stenosis Grades, Conversion and Management
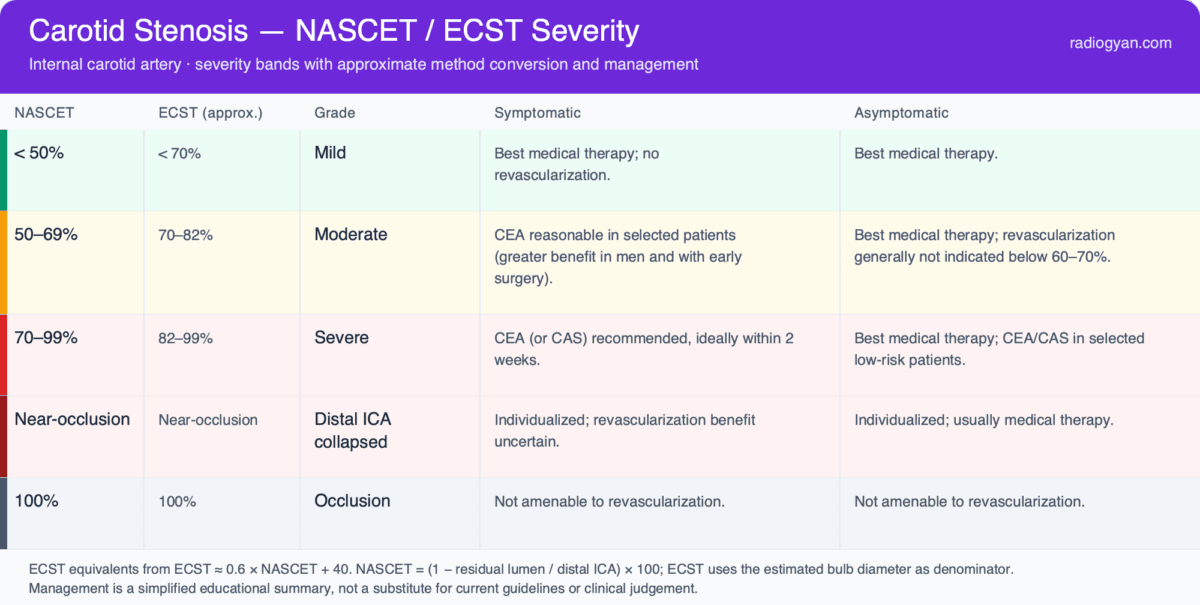
| NASCET | ECST (approx.) | Grade | Symptomatic management | Asymptomatic management |
|---|---|---|---|---|
| < 50% | < 70% | Mild | Best medical therapy; no revascularization | Best medical therapy |
| 50–69% | 70–82% | Moderate | CEA reasonable in selected patients (greater benefit in men and with early surgery) | Best medical therapy; revascularization generally not indicated below 60–70% |
| 70–99% | 82–99% | Severe | CEA (or CAS) recommended, ideally within 2 weeks | Best medical therapy; CEA/CAS in selected low-risk patients |
| Near-occlusion | Near-occlusion | Distal ICA collapsed | Individualized; revascularization benefit uncertain | Individualized; usually medical therapy |
| 100% | 100% | Occlusion | Not amenable to revascularization | Not amenable to revascularization |
Doppler Ultrasound Criteria (SRU Consensus)
When stenosis is graded by carotid duplex, the calculator uses the Society of Radiologists in Ultrasound (SRU) 2003 consensus criteria, which map ICA velocities to NASCET-method categories. The ICA peak systolic velocity (PSV) is the primary parameter; the ICA/CCA PSV ratio and the ICA end-diastolic velocity (EDV) are confirmatory and are especially useful when the PSV is borderline, when there is contralateral high-grade disease, or when cardiac output is abnormal.
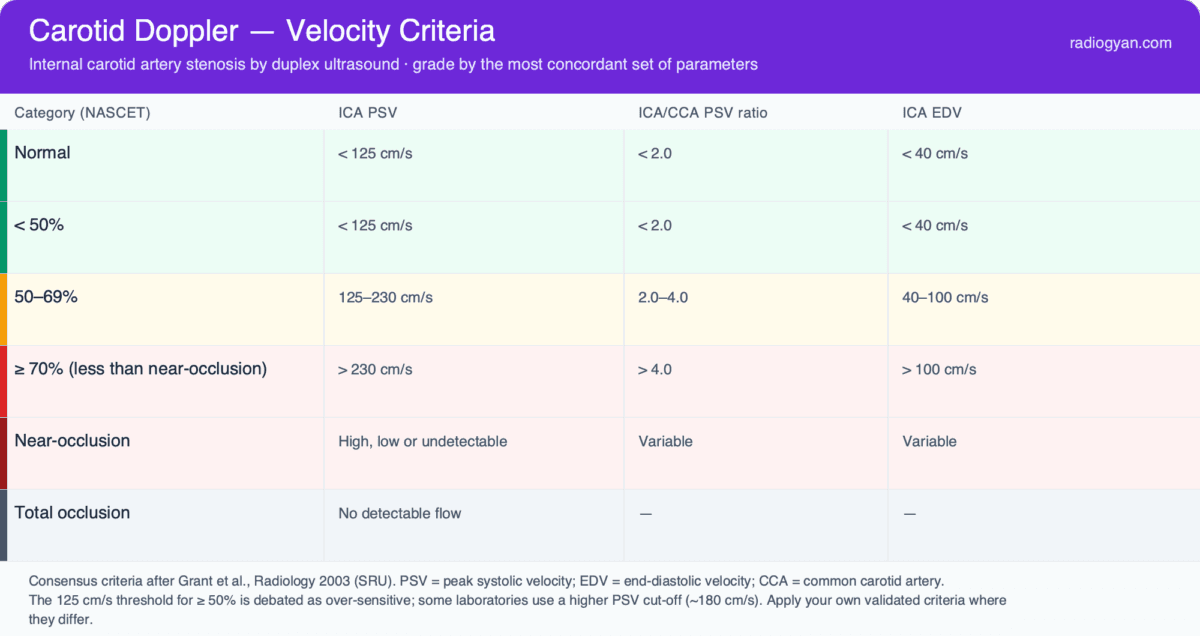
| Category (NASCET) | ICA PSV | ICA/CCA PSV ratio | ICA EDV |
|---|---|---|---|
| Normal | < 125 cm/s | < 2.0 | < 40 cm/s |
| < 50% | < 125 cm/s | < 2.0 | < 40 cm/s |
| 50–69% | 125–230 cm/s | 2.0–4.0 | 40–100 cm/s |
| ≥ 70% (less than near-occlusion) | > 230 cm/s | > 4.0 | > 100 cm/s |
| Near-occlusion | High, low or undetectable | Variable | Variable |
| Total occlusion | No detectable flow | — | — |
Carotid Near-Occlusion: A Special Case
In a critical stenosis the post-stenotic pressure drop can cause the distal ICA to collapse, producing the angiographic “string sign.” Because the NASCET denominator (the distal ICA) is itself narrowed, the calculated percentage under-estimates the true severity — a near-occlusion may compute as only 80–90% yet be functionally near-complete. On ultrasound, velocities are unreliable and may be paradoxically low. Near-occlusion is therefore reported as a distinct category rather than a number, and its management differs: the benefit of revascularization is uncertain and many patients are managed medically. Flag the near-occlusion checkbox whenever the distal lumen is collapsed.
Reporting Tips and Common Pitfalls
- State the method. A bare “75% stenosis” is ambiguous — always specify NASCET or ECST, because the same lesion differs by roughly 10–20 percentage points between them.
- Choose the NASCET reference correctly. Measure the distal ICA where the walls are parallel, beyond any post-bulbar widening; measuring too proximally inflates the denominator and the percentage.
- Watch for near-occlusion. A collapsed distal ICA makes the NASCET ratio under-read; recognise the string sign and report it as near-occlusion.
- Correlate discordant ultrasound parameters. If the PSV, the ratio and the EDV disagree, or if there is contralateral occlusion, confirm with CTA or MRA before committing to a grade.
- Tie the grade to the clinical context. The decision to revascularize hinges on symptomatic status, sex, timing from the event and peri-operative risk — not on the percentage alone.
Frequently Asked Questions
How is NASCET measured?
NASCET % = (1 − minimal residual lumen ÷ normal distal ICA diameter) × 100. The numerator is the narrowest luminal diameter at the stenosis; the denominator is the diameter of the disease-free distal cervical ICA, measured well beyond the bulb where the walls are parallel — never within the bulb or a post-stenotic dilated segment, both of which inflate the denominator and overcall the stenosis. The method applies to DSA, CTA and contrast-enhanced MRA alike; measure on the projection or reformat showing the tightest narrowing.
What are the NASCET criteria for grading carotid stenosis?
The trial-derived severity bands are: <50% mild, 50–69% moderate, 70–99% severe, plus near-occlusion (collapsed or threadlike distal ICA — the percentage is unreliable here and the finding should be named morphologically) and total occlusion. These cut-points matter because NASCET showed a clear endarterectomy benefit for symptomatic 70–99% stenosis and a moderate benefit at 50–69%; the same NASCET-referenced bands underpin the SRU Doppler velocity criteria.
What is the difference between NASCET and ECST?
Both grade the same carotid stenosis but against different reference diameters. NASCET uses the normal ICA distal to the stenosis as the denominator, while ECST uses the estimated original diameter of the carotid bulb at the stenosis. ECST therefore gives a higher percentage; the two are related by ECST ≈ 0.6 × NASCET + 40.
How do I convert ECST to NASCET, or NASCET to ECST?
Use ECST ≈ (0.6 × NASCET) + 40, or rearranged, NASCET ≈ (ECST − 40) / 0.6. A NASCET 70% equals about ECST 82%, and ECST 70% equals about NASCET 50%. The calculator performs this conversion automatically when only one reference diameter is entered.
Which method do current guidelines and ultrasound criteria use?
Contemporary guidelines and the SRU Doppler velocity criteria are based on the NASCET method, which is the recommended standard for correlating ultrasound with angiography. ECST values are still encountered in European reports and older literature, so understanding both remains important.
When is carotid endarterectomy indicated?
For symptomatic patients, endarterectomy clearly benefits 70–99% (NASCET) stenosis and offers moderate benefit at 50–69%, particularly in men, with recent symptoms, and when performed early at a low-risk centre. For asymptomatic patients, the benefit is smaller and is generally limited to selected, low-surgical-risk individuals with high-grade stenosis; many are managed with optimal medical therapy alone. These are educational summaries — consult current guidelines for definitive thresholds.
What ICA velocity indicates a 50% or 70% carotid stenosis?
By the SRU criteria, a 50–69% (NASCET) stenosis corresponds to an ICA PSV of 125–230 cm/s with an ICA/CCA ratio of 2.0–4.0 and EDV 40–100 cm/s; ≥ 70% corresponds to PSV > 230 cm/s, ratio > 4.0 and EDV > 100 cm/s. PSV is the primary parameter, with the ratio and EDV confirmatory when the PSV is borderline or contralateral high-grade disease elevates flow. Near-occlusion can drop velocities paradoxically and must be graded on morphology, not velocity.
References
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. New England Journal of Medicine. 1991;325(7):445–453.
- European Carotid Surgery Trialists’ Collaborative Group. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351(9113):1379–1387.
- Rothwell PM, Gibson RJ, Slattery J, Warlow CP. Equivalence of measurements of carotid stenosis: a comparison of three methods on 1001 angiograms. Stroke. 1994;25(12):2435–2439.
- Grant EG, Benson CB, Moneta GL, et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis — Society of Radiologists in Ultrasound consensus conference. Radiology. 2003;229(2):340–346.
- Polak JF, et al. Accuracy of the Society of Radiologists in Ultrasound (SRU) carotid Doppler velocity criteria for grading NASCET stenosis: a meta-analysis. Journal of Ultrasound in Medicine. 2023.
This calculator implements the NASCET and ECST measurement methods, the Rothwell conversion and the SRU Doppler consensus; in case of any discrepancy, the original publications and current clinical guidelines take precedence.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
About the Author
Dr. Amar Udare, MD, DNB
Dr. Udare holds an MBBS and MD degree, and his expertise lies in the field of radiology. He has authored multiple peer-reviewed publications, contributing significantly to the medical field. His works can be accessed on PubMed and Google Scholar.
In addition to his academic and professional achievements, Dr. Udare is an avid reader and enjoys exploring the latest advancements in medical technology. His commitment to making complex medical knowledge accessible to patients and the general public aligns with our mission at RadioGyan.com.
For any further questions or clarifications, feel free to reach out to Dr. Udare via the contact form.