
| Non-rim APHE | Size | 0 add’l features | 1 add’l feature | ≥ 2 add’l features |
|---|---|---|---|---|
| Absent | < 20 mm | LR-3 | LR-3 | LR-4 |
| ≥ 20 mm | LR-3 | LR-4 | LR-4 | |
| Additional major features = non-peripheral washout, enhancing capsule, threshold growth | ||||
| Present | < 10 mm | LR-3 | LR-4 | LR-4 |
| 10–19 mm | LR-4 | LR-5 | LR-5 | |
| ≥ 20 mm | LR-4 | LR-5 | LR-5 | |
| Non-rim APHE | Size | No washout | Late (≥60 s) & mild washout |
|---|---|---|---|
| Absent | < 10 mm | LR-3 | LR-3 |
| 10–19 mm | LR-3 | LR-4 | |
| ≥ 20 mm | LR-3 | LR-4 | |
| Present | < 10 mm | LR-3 | LR-4 |
| 10–19 mm | LR-4 | LR-5 | |
| ≥ 20 mm | LR-4 | LR-5 | |
| Rim APHE, early (<60 s) washout, or marked washout → LR-M | |||
| Category | Definition | Management |
|---|---|---|
| US-1 | Negative — no observation or definitely benign | Routine surveillance US ± AFP in 6 months |
| US-2 | Subthreshold — observation < 10 mm | Short-interval US in 3–6 months |
| US-3 | Positive — ≥ 10 mm or new thrombus | Diagnostic CT/MRI or CEUS (multiphase) |
| VIS-C | Severe limitation modifier | Repeat US in 3 months ×1 or alternative surveillance |
| Category | Non-radiation | Radiation |
|---|---|---|
| Nonviable | No masslike enhancement | No masslike enhancement |
| Equivocal | Uncertain masslike enhancement | — (not used) |
| Nonprogressing | — (not used) | Masslike enhancement, stable / decreasing |
| Viable | Masslike enhancement present | Masslike enhancement, new / increasing |
| Perilesional ↓ / Intralesional → | Absent | Uncertain | Present |
|---|---|---|---|
| Absent | Nonviable | Equivocal | Viable |
| Uncertain | Equivocal | Equivocal | Viable |
| Present | Viable | Viable | Viable |
This tool implements ACR LI-RADS® CT/MRI v2018, CEUS, US Surveillance v2024, and CT/MRI and CEUS Treatment Response v2024. Final classification and management must be made by a qualified radiologist using the full imaging study and clinical context.
LI-RADS® 2024 Calculator for CT/MRI, CEUS, US and Treatment Response
This LI-RADS calculator assigns the correct Liver Imaging Reporting and Data System category for liver observations in patients at risk for hepatocellular carcinoma (HCC), and generates an editable, dictation-ready report. It implements all four current ACR algorithms in one interface: CT/MRI Diagnostic v2018, CEUS Diagnostic, US Surveillance v2024, and the bifurcated CT/MRI Treatment Response (TRA) v2024.
Enter the imaging features and the tool returns the category, the approximate likelihood of HCC, the recommended management, and a structured report you can paste into PowerScribe, RadAI or any reporting system. The diagnostic logic follows the ACR CT/MRI diagnostic table exactly, including the size and major-feature thresholds that separate LR-3, LR-4 and LR-5.
Which Algorithm Applies?
- US Surveillance v2024 – screening ultrasound. Reports a US category (US-1/2/3) plus a visualization score (VIS-A/B/C), with AFP folded into management.
- CT/MRI Diagnostic v2018 – multiphase contrast-enhanced CT or MRI (extracellular or hepatobiliary agent) to characterise an observation.
- CEUS Diagnostic – contrast-enhanced ultrasound with a pure intravascular microbubble agent.
- Treatment Response v2024 – a treated lesion after locoregional therapy or at a surgical margin, using the appropriate non-radiation or radiation algorithm.
CT/MRI Major Features and the Diagnostic Table
The CT/MRI category is a function of observation size, the presence of non-rim arterial phase hyperenhancement (APHE), and the count of additional major features: non-peripheral “washout,” enhancing “capsule,” and threshold growth. All three additional features are weighted equally when counting toward LR-3/4/5.
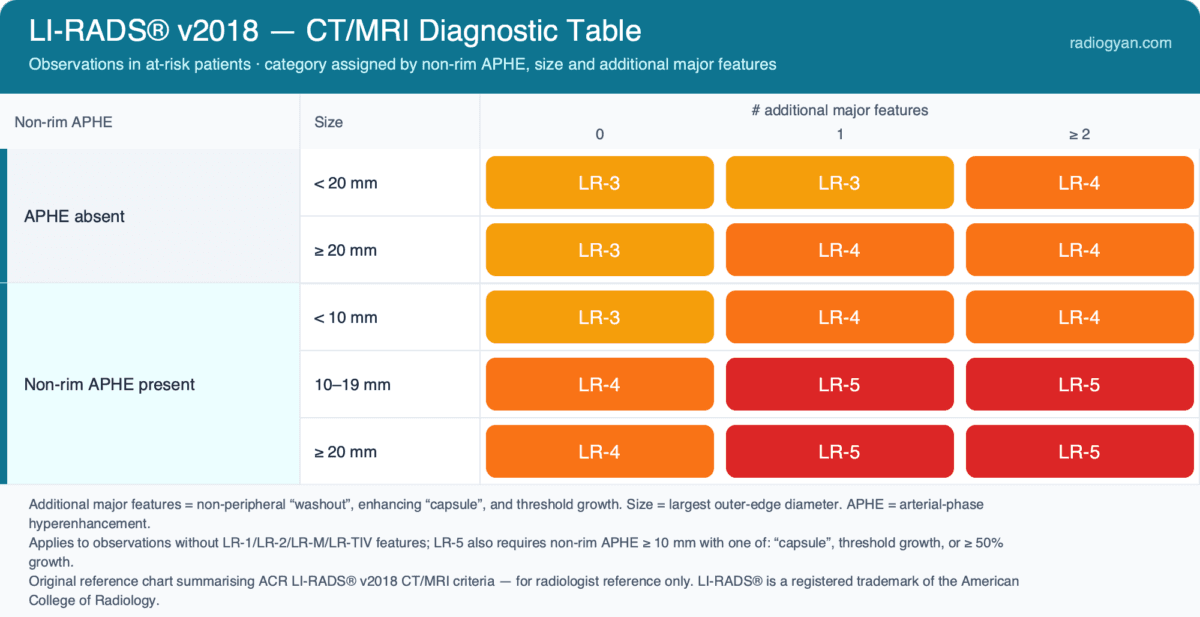
| Non-rim APHE | Size | 0 features | 1 feature | ≥2 features |
|---|---|---|---|---|
| Absent | <20 mm | LR-3 | LR-3 | LR-4 |
| Absent | ≥20 mm | LR-3 | LR-4 | LR-4 |
| Present | <10 mm | LR-3 | LR-4 | LR-4 |
| Present | 10–19 mm | LR-4 | LR-5 | LR-5 |
| Present | ≥20 mm | LR-4 | LR-5 | LR-5 |
Note the two structural rules that catch readers out: an observation can only reach LR-5 if it is ≥10 mm with non-rim APHE plus at least one additional major feature, and a sub-centimetre APHE-positive nodule can never exceed LR-4. The calculator enforces these automatically.
Categories and Approximate HCC Likelihood
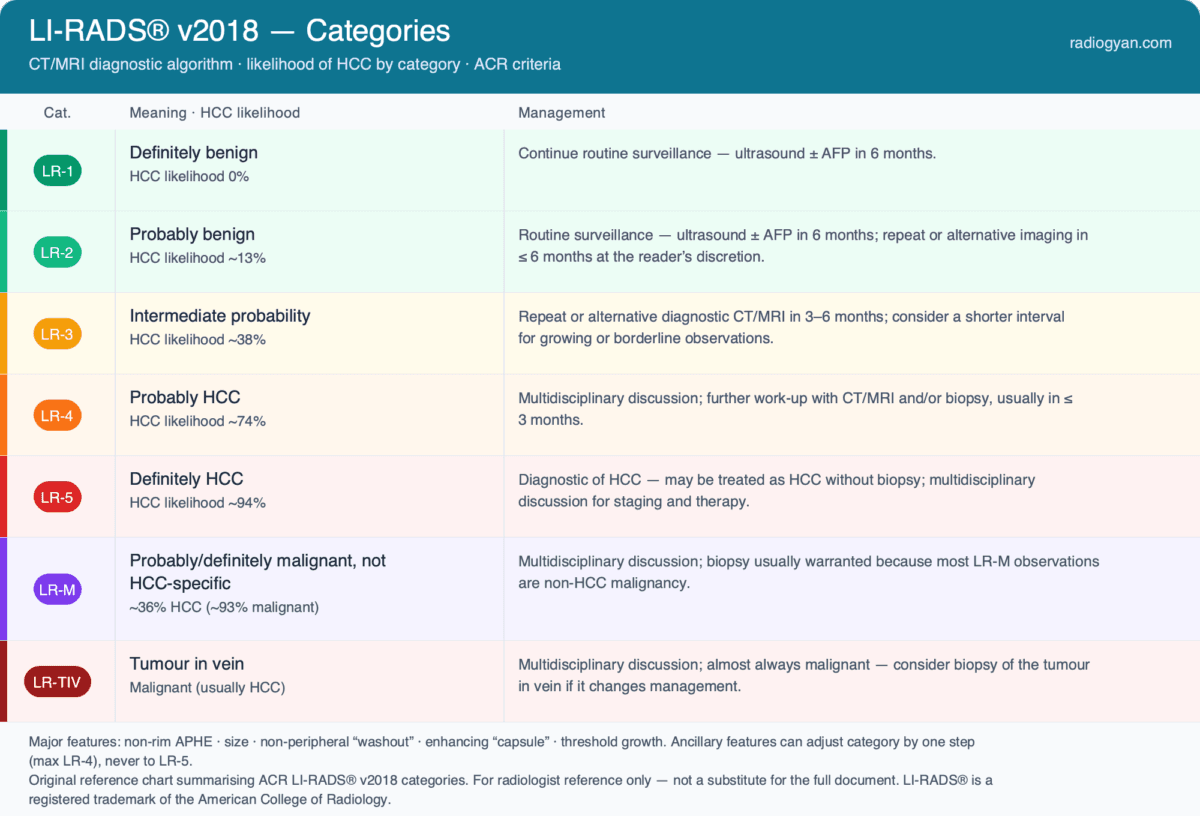
| Category | Meaning | HCC likelihood |
|---|---|---|
| LR-1 | Definitely benign | 0% |
| LR-2 | Probably benign | ~13% |
| LR-3 | Intermediate probability | ~38% |
| LR-4 | Probably HCC | ~74% |
| LR-5 | Definitely HCC | ~94% |
| LR-M | Probably/definitely malignant, not HCC-specific | ~36% HCC (~93% malignant) |
| LR-TIV | Tumor in vein | Malignant (usually HCC) |
Applying Ancillary Features (LR-3 vs LR-4)
Ancillary features are optional and used to adjust, never to override, the major-feature category. Features favouring malignancy (nodule-in-nodule, mosaic architecture, fat or blood products in mass, restricted diffusion, mild–moderate T2 hyperintensity, corona enhancement, transitional- or hepatobiliary-phase hypointensity) can upgrade by one or more categories up to a ceiling of LR-4 — they can never produce an LR-5. Features favouring benignity (size stability ≥2 years, marked T2 hyperintensity, hepatobiliary-phase isointensity, iron in mass) can downgrade. When features point in both directions, no net adjustment is made. The most common practical use is nudging a borderline LR-3 to LR-4.
Threshold Growth and Comparison With Priors
Threshold growth is a ≥50% increase in diameter within ≤6 months and counts as a major feature. The calculator includes a prior-comparison helper: enter the prior size and interval and it computes the percentage change, applies threshold growth automatically when the definition is met, and flags a ≥50% increase over a longer interval as sub-threshold growth — which is an ancillary feature favouring malignancy rather than a major feature. This directly addresses interval change, which is otherwise easy to mis-handle.
CEUS: Washout Timing and Degree
CEUS uses the same APHE-plus-size-plus-washout logic but with washout characterised by onset and degree. Only late (≥60 s) and mild washout supports the HCC pathway; early (<60 s) washout or marked (“punched-out”) washout, and rim APHE, instead categorise the nodule as CEUS LR-M. Because microbubble agents are purely intravascular, CEUS is particularly useful for resolving washout when CT/MRI is equivocal, and the calculator routes these washout subtypes to the correct category.
US Surveillance v2024
Surveillance ultrasound is reported with a category and a visualization score. US-1 (negative) returns to routine 6-month surveillance; US-2 (subthreshold observation <10 mm) prompts short-interval ultrasound in 3–6 months; US-3 (observation ≥10 mm not definitely benign, or new venous thrombus) prompts multiphase diagnostic CT, MRI or CEUS. The visualization score — VIS-A (none/minimal), VIS-B (moderate), VIS-C (severe) — conveys expected sensitivity. The 2024 update folds AFP and VIS-C into post-examination management: a positive or rising AFP after a non-positive ultrasound, or a VIS-C study, escalates to a shorter interval or an alternative modality.
Treatment Response v2024: Two Algorithms
CT/MRI TRA v2024 splits into separate cores by mechanism. The non-radiation algorithm (RFA, MWA, cryoablation, PEI, TAE, cTACE, DEB-TACE, and surgical margins) uses LR-TR Nonviable / Equivocal / Viable, with viability now hinging on a single feature: masslike enhancement of any degree in any phase. The radiation algorithm (TARE, SBRT) replaces Equivocal with LR-TR Nonprogressing — stable or decreasing masslike enhancement — because irradiated HCC can enhance for months before regressing, so persistent enhancement alone should not be called viable. In both, diffusion restriction or mild–moderate T2 hyperintensity in the area of uncertain or non-progressing enhancement may optionally upgrade to LR-TR Viable.
A separate CEUS Nonradiation TRA v2024 algorithm applies to lesions treated by TACE, TAE, RFA, MWA, PEA or resection and imaged with contrast-enhanced ultrasound. It assesses intralesional and perilesional tumour viability separately — each graded absent, uncertain or present using CEUS enhancement and washout criteria — and reconciles them into a single LR-TR Nonviable, Equivocal or Viable category. The calculator implements this two-axis grid in full, including LR-TR Nonevaluable for non-diagnostic studies.
What’s New in LI-RADS 2024
- CT/MRI Treatment Response split into separate non-radiation and radiation cores.
- New LR-TR Nonprogressing category for the radiation algorithm; single-feature definition of viability.
- Optional ancillary-feature upgrade to LR-TR Viable; non-radiation algorithm now applicable to surgical margins.
- US Surveillance v2024 incorporates AFP and the VIS-C score into management, improving sensitivity over the 2017 version.
Reporting Tips and Common Pitfalls
- Measure the observation at its largest outer-edge dimension on the sequence and phase where margins are clearest; exclude capsule and perilesional enhancement from the measurement.
- Rim APHE, peripheral washout and delayed central enhancement are targetoid features — assign LR-M, not the HCC pathway, and consider biopsy.
- Do not call washout in the hepatobiliary phase with a gadoxetate agent; restrict washout assessment to the portal-venous phase for HBA.
- Unequivocal enhancing soft tissue in a vein is LR-TIV regardless of whether a parenchymal mass is seen, and is a contraindication to transplantation.
- When uncertain between two categories, assign the one reflecting lower certainty.
Frequently Asked Questions
Which patients is LI-RADS applied to?
Adults at high risk for HCC: cirrhosis of any cause except certain vascular and congenital aetiologies, chronic hepatitis B without cirrhosis, and current or prior HCC, including liver transplant candidates and recipients. It is not applied to patients younger than 18, those without these risk factors, or cirrhosis from congenital hepatic fibrosis or vascular disorders such as Budd-Chiari or cardiac congestion.
Can LR-5 be treated as HCC without biopsy?
Yes. LR-5 is a noninvasive diagnosis of HCC in an appropriate at-risk patient and aligns with OPTN class-5 criteria used for transplant prioritisation. Management is typically determined at a multidisciplinary tumour board.
What separates LR-5 from LR-M?
LR-5 is definite HCC. LR-M is probably or definitely malignant but not specific for HCC — a targetoid mass or an infiltrative, markedly diffusion-restricting lesion that may represent intrahepatic cholangiocarcinoma or combined HCC-CCA. Most LR-M lesions are biopsied, since misclassifying them as HCC can alter transplant eligibility and treatment.
What is threshold growth in LI-RADS?
Threshold growth is a ≥ 50% increase in observation diameter within ≤ 6 months and counts as a major feature toward LR-4/LR-5. A ≥ 50% increase over a longer interval is sub-threshold growth — an ancillary feature favouring malignancy, not a major feature — and on its own cannot push an observation to LR-5.
References
- American College of Radiology. LI-RADS® – Liver Imaging Reporting and Data System. Reston, VA: ACR (current manuals and Core documents).
- Chernyak V, Fowler KJ, Kamaya A, et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology. 2018;289(3):816–830.
- Wilson SR, Lyshchik A, Piscaglia F, et al. CEUS LI-RADS: algorithm, implementation, and key differences from CT/MRI. Abdominal Radiology. 2018;43(1):127–142.
- Kamaya A, Fetzer DT, Seow JH, et al. LI-RADS US Surveillance Version 2024 for Surveillance of Hepatocellular Carcinoma: An Update to the American College of Radiology US LI-RADS. Radiology. 2024;312(2):e240169.
- CT/MRI LI-RADS 2024 Update: Treatment Response Assessment. Radiology. 2024; doi:10.1148/radiol.232408.
- Lyshchik A, Fetzer DT, Kono Y, et al. Liver Imaging Reporting and Data System Contrast-Enhanced US Nonradiation Treatment Response Assessment Version 2024. Radiology. 2024;311(2):e232369.
- LI-RADS in 2024: recent updates, planned refinements, and future directions. Abdominal Radiology. 2024.
This calculator implements the algorithms as published by the ACR; in case of any discrepancy, the official ACR LI-RADS® manuals and Core documents take precedence.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
About the Author
Dr. Amar Udare, MD, DNB
Dr. Udare holds an MBBS and MD degree, and his expertise lies in the field of radiology. He has authored multiple peer-reviewed publications, contributing significantly to the medical field. His works can be accessed on PubMed and Google Scholar.
In addition to his academic and professional achievements, Dr. Udare is an avid reader and enjoys exploring the latest advancements in medical technology. His commitment to making complex medical knowledge accessible to patients and the general public aligns with our mission at RadioGyan.com.
For any further questions or clarifications, feel free to reach out to Dr. Udare via the contact form.