
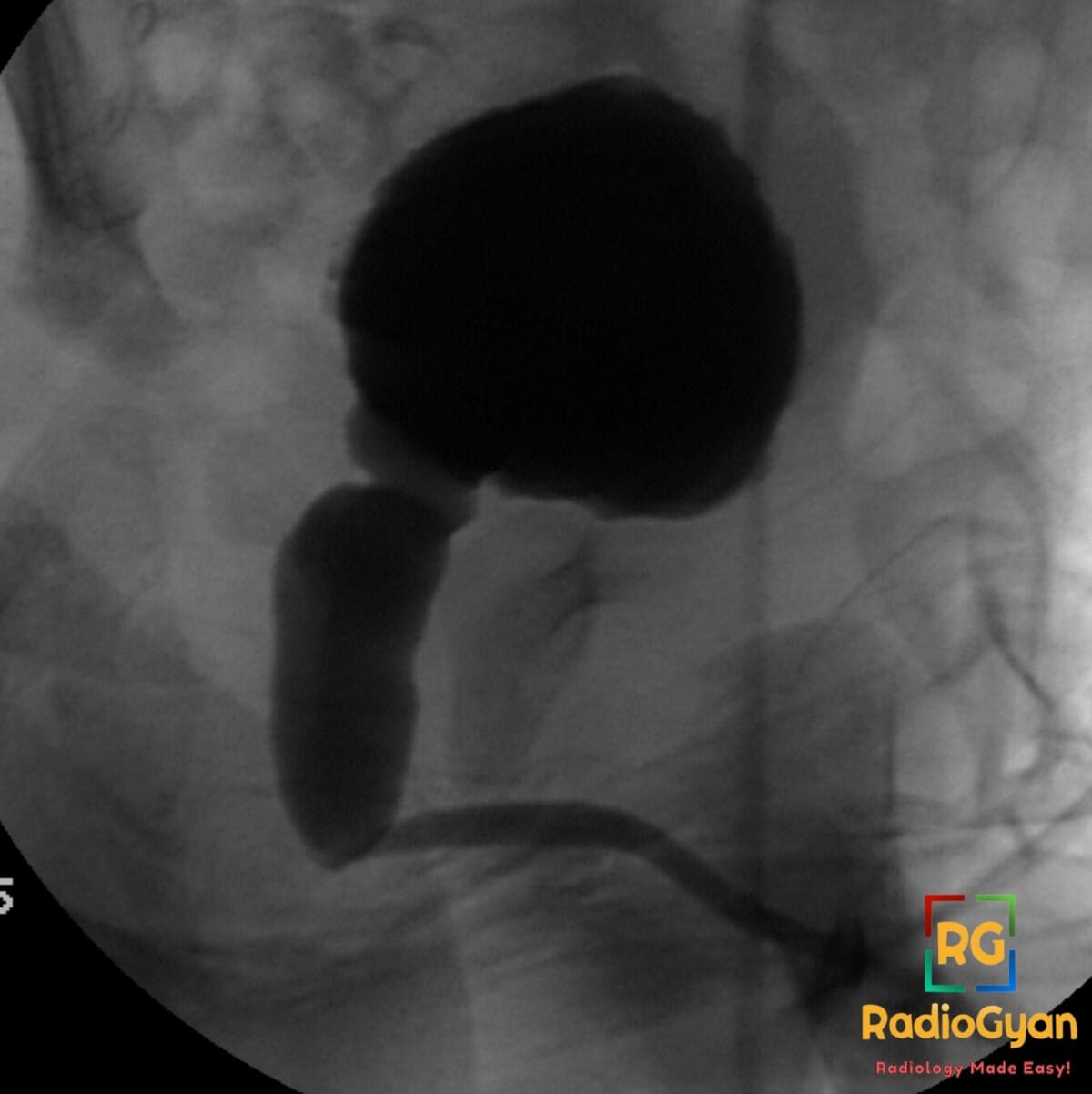
1 month old male presenting with a poor urinary stream and a palpable midline abdominal mass.
Diagnosis and teaching points:
Diagnosis: Posterior urethral valves (PUV) with marked posterior urethral dilation and abrupt caliber change
Key facts for boards exams:
- Most common cause of bladder outlet obstruction in male infants and a leading cause of pediatric renal failure.
- VCUG is the gold standard diagnostic study, typically performed during the voiding phase to demonstrate the posterior urethral anatomy.
- The “keyhole sign” on ultrasound or VCUG represents the dilated posterior urethra and thickened bladder.
- Classified by Young’s criteria, with Type 1 (folds extending distally from the verumontanum) being the most common.
- Vesicoureteral reflux (VUR) is present in approximately 50% of cases due to high intravesical pressures.
Detailed teaching points:
- Clinical: Exclusively affects male infants; often presents via prenatal hydronephrosis, or postnatally with poor urinary stream, dribbling, palpable bladder, or recurrent UTIs.
- Etiology/Pathophys: Maldevelopment of mucosal folds in the posterior urethra (Type 1 or Type 3/Cobb’s collar) creates an obstruction that leads to proximal urethral dilation, bladder wall hypertrophy/trabeculation, and upstream hydroureteronephrosis.
- Radiograph: VCUG during voiding phase shows marked dilation of the posterior urethra (>6 mm), an elongated posterior urethra, and an abrupt caliber change at the valve site. A thick-walled, trabeculated bladder and VUR are frequent secondary findings.
- US: Shows the “keyhole sign” (dilated posterior urethra and bladder), bladder wall thickening, hydroureteronephrosis, and potentially oligohydramnios in the prenatal setting.
- CT: Not primary modality; shows similar findings of dilated posterior urethra, bladder thickening, and hydroureteronephrosis.
- MRI: Primarily used for complex anatomy or assessing renal dysplasia; shows urethral dilation and bladder trabeculation.
- Nuc Med: DMSA is used to evaluate renal scarring or differential function; MAG3/DTPA renography assesses the degree of obstruction and drainage.
- Signs: Keyhole sign: The combination of a dilated posterior urethra and a distended bladder. Dilated posterior urethra with abrupt caliber change: Pathognomonic VCUG finding for valve obstruction.
- Frameworks: Young Classification: Type 1 (posterolateral folds), Type 2 (clinically insignificant), and Type 3 (circular diaphragm below verumontanum).
- DDx: Urethral atresia (complete obstruction, rarer); Anterior urethral valve (dilation in penile/anterior urethra); Spinning top urethra (nonobstructive widening in older boys, no abrupt caliber change); Urethral polyp/stricture (focal filling defect).
- Tx: Standard definitive treatment is endoscopic valve ablation (transurethral resection); temporary measures include vesicostomy or catheter drainage if the infant is too small or unstable for surgery.
OSCE Questions
Question: What is the gold standard imaging modality for the diagnosis of this condition?
Voiding cystourethrogram (VCUG).
Question: Which ultrasound finding, consisting of a dilated posterior urethra and bladder, is highly suggestive of this pathology?
The keyhole sign.
Question: What is the most common anatomic subtype of this condition according to the Young classification system?
Type 1, characterized by posterolateral folds extending distally from the verumontanum.
Question: What secondary vesicoureteral finding is observed in approximately 50% of patients with this pathology?
Vesicoureteral reflux (VUR).
Question: What is the definitive surgical treatment for an infant diagnosed with this condition?
Endoscopic valve ablation or fulguration.
MCQ Questions
1. What is the gold standard imaging study for this diagnosis?
A. Renal ultrasound
B. Voiding cystourethrogram (VCUG)
C. Non-contrast CT abdomen
D. DMSA renal scan
Answer: B. Voiding cystourethrogram (VCUG). VCUG is the definitive study as it allows direct visualization of the posterior urethra during the voiding phase.
2. Which sonographic finding is highly suggestive of this condition?
A. Spinning top sign
B. Keyhole sign
C. Target sign
D. Mickey Mouse sign
Answer: B. Keyhole sign. This sign represents the combination of a dilated bladder and a dilated posterior urethra on ultrasound.
3. What is the most common embryologic subtype of this pathology?
A. Type 1
B. Type 2
C. Type 3
D. Type 4
Answer: A. Type 1. Type 1 valves, which are posterolateral mucosal folds, are the most frequently encountered subtype in clinical practice.
4. Which patient population is almost exclusively affected by this condition?
A. Female neonates
B. Adolescent females
C. Male infants
D. Elderly males
Answer: C. Male infants. This condition is a congenital obstructive anomaly that occurs specifically in males.
5. What is the most common associated finding in the upper urinary tract?
A. Urethral atresia
B. Anterior urethral webs
C. Vesicoureteral reflux
D. Polycystic kidney disease
Answer: C. Vesicoureteral reflux. Vesicoureteral reflux occurs in approximately 50% of patients due to high intravesical pressures.
Check out more such cases:






Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case