
Routine second trimester screening ultrasound in a 28-year-old pregnant female.
Diagnosis and teaching points:
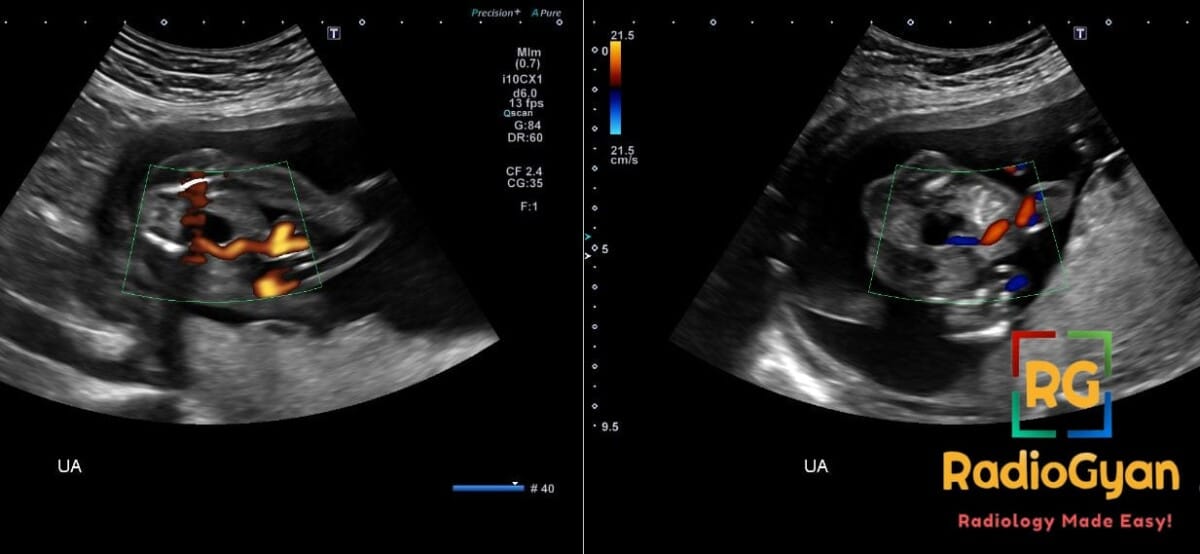
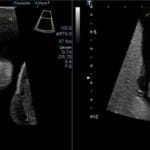
Diagnosis: Single Umbilical Artery (SUA)
Key facts for boards exams:
- SUA is the most common umbilical cord anomaly, occurring in 0.5–6% of singleton pregnancies and up to 5% of twin pregnancies.
- While isolated SUA usually has a favorable prognosis, its presence with other structural anomalies increases the risk of chromosomal abnormalities (especially Trisomy 13 and 18) to approximately 50%.
- Management of isolated SUA requires serial third-trimester ultrasounds to monitor for fetal growth restriction (FGR) and antenatal testing beginning at 36 weeks due to a twofold increase in stillbirth risk.
Detailed teaching points:
- Clinical: Occurs prenatally; no maternal symptoms; associated with fetal growth restriction (10% lower birth weight) and increased risk of stillbirth; higher prevalence in twins.
- Etiology/Pathophys: Results from the absence of one umbilical artery, leading to a two-vessel cord (one vein, one artery); likely caused by the failure of the umbilical artery to split during the first month of gestation.
- US: Primary diagnostic tool; hallmark finding is visualization of only one artery coursing around the fetal bladder in cross-section; two-vessel cord appearance instead of normal three-vessel cord; 84% sensitive in the first trimester.
- MRI: Not routinely used; may be considered for detailed fetal anatomic assessment if ultrasound findings are equivocal.
- Signs: Single Artery Around the Fetal Bladder sign (diagnostic hallmark); may see associated signs like increased nuchal translucency or hydronephrosis if non-isolated.
- Frameworks: SMFM guidelines for isolated SUA recommend no additional aneuploidy screening if isolated, but require serial growth ultrasounds and fetal heart rate monitoring starting at 36 0/7 weeks.
- DDx: Isolated SUA (benign); SUA with associated chromosomal abnormalities (Trisomy 13, 18, or Triploidy); rare two-vessel cord anatomic variants.
- Tx: Detailed anatomy ultrasound to rule out associated defects; serial growth scans in the third trimester; genetic counseling/amniocentesis if other anomalies are found; vaginal delivery is appropriate with close monitoring.
OSCE Questions
Question: What is the most common ultrasound sign used to confirm this pathology in the fetal pelvis?
Visualization of only one umbilical artery lateral to the fetal bladder.
Question: Which two chromosomal trisomies are most frequently associated with this condition when structural anomalies are present?
Trisomy 13 and Trisomy 18.
Question: What is the recommended management for a fetus with an isolated third-trimester finding of this pathology?
Serial ultrasounds for growth assessment and antenatal testing starting at 36 weeks gestation.
Question: Beyond chromosomal issues, what fetal growth complication is associated with this condition?
Fetal growth restriction (FGR).
Question: This condition occurs more frequently in which type of pregnancy gestation?
Twin pregnancies.
MCQ Questions
1. What is the classic ultrasound sign of this pathology?
A. Two arteries around the bladder
B. One artery around the bladder
C. Two veins near the bladder
D. Reversed venous flow
Answer: B. One artery around the bladder. The hallmark ultrasound finding is visualizing only one umbilical artery instead of two adjacent to the fetal bladder.
2. This finding is most strongly associated with which chromosomal abnormalities?
A. Trisomy 21 and 16
B. Trisomy 13 and 18
C. Turner syndrome
D. Klinefelter syndrome
Answer: B. Trisomy 13 and 18. When additional structural anomalies are present, the risk for Trisomy 13 and 18 increases to approximately 50%.
3. Which growth complication is associated with this umbilical cord finding?
A. Macrosomia
B. Polyhydramnios
C. Fetal growth restriction
D. Hydrops fetalis
Answer: C. Fetal growth restriction. This pathology is associated with an increased risk of fetal growth restriction and lower average birth weights.
4. What is the recommended management for the isolated form of this pathology?
A. Immediate cesarean delivery
B. First trimester amniocentesis
C. Third trimester growth ultrasounds
D. Termination of pregnancy
Answer: C. Third trimester growth ultrasounds. Serial ultrasounds are recommended in the third trimester to monitor for fetal growth restriction in isolated cases.
5. At what gestational age is antenatal testing typically initiated for this condition?
A. 20 weeks
B. 28 weeks
C. 32 weeks
D. 36 weeks
Answer: D. 36 weeks. Antenatal fetal heart rate monitoring is recommended to begin at 36 weeks for isolated cases due to stillbirth risks.
Check out more such cases:





Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case