
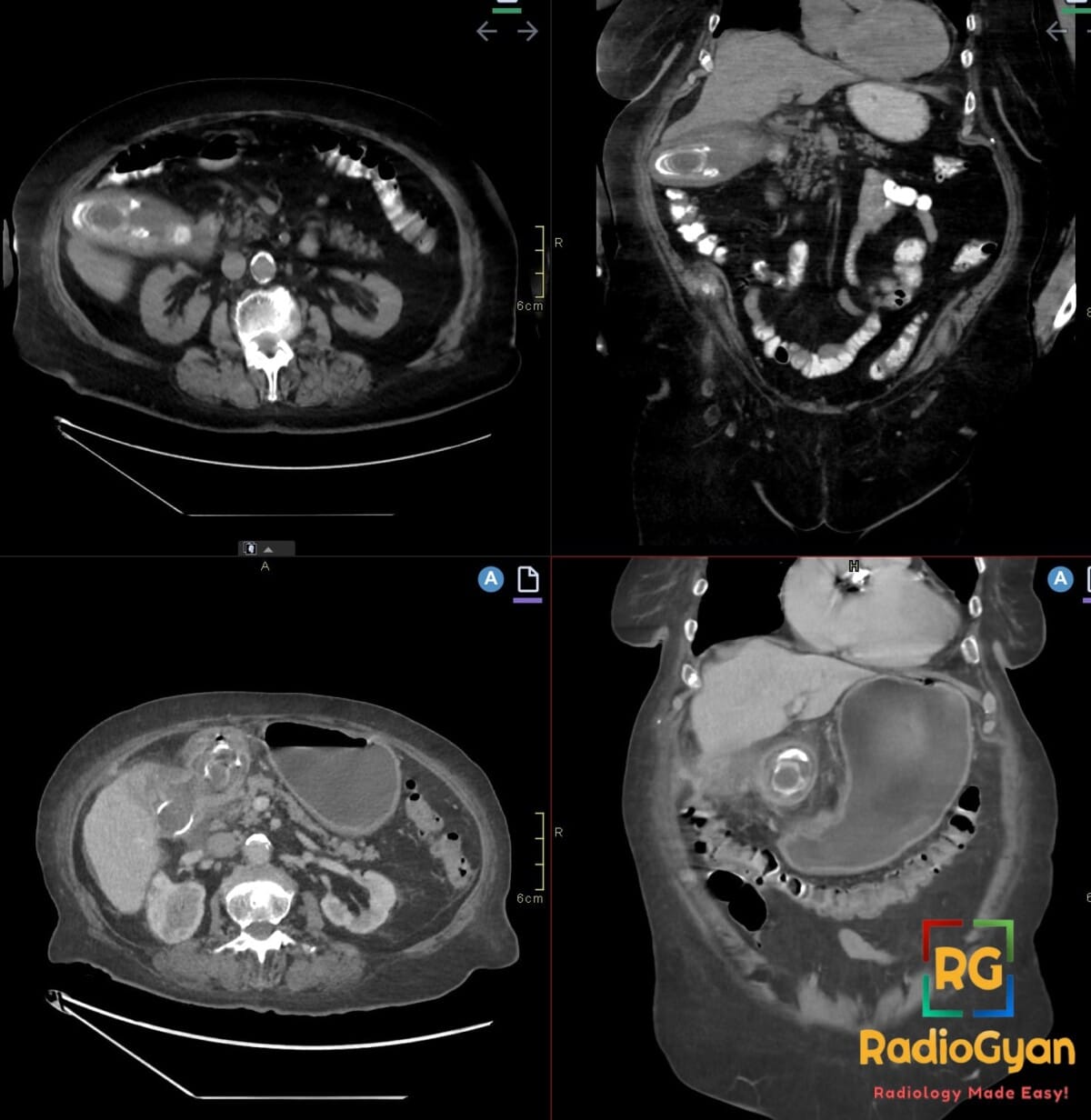
75-year-old female presenting with nausea, vomiting, and abdominal pain. What is your diagnosis?
Diagnosis and teaching points:
Diagnosis: Bouveret syndrome. CT shows gallbladder calculi. Gastric outlet obstruction is secondary to gallstones fistulizing into the lumen.
Key facts for board exams:
- Rare variant of gallstone ileus causing gastric outlet obstruction via a cholecystoduodenal fistula
- Demographics: elderly women (6th–8th decade) with longstanding cholelithiasis and chronic cholecystitis
- Imaging triad: pneumobilia, bowel obstruction, ectopic gallstone (Rigler triad), with the stone lodged in the pylorus or proximal duodenum
- CT is the diagnostic modality of choice and directly demonstrates the fistula and impacted stone
- Management is typically endoscopic or surgical stone extraction with repair of the biliary-enteric fistula; morbidity and mortality are high due to advanced age and comorbidities
Detailed teaching points:
- Clinical: Elderly women (mean age ~70); presents with nausea, non-bilious vomiting, epigastric pain, early satiety, and weight loss; accounts for <5% of all gallstone ileus cases
- Etiology/Pathophys: Chronic cholecystitis causes the gallbladder to adhere to and erode into the adjacent GI tract (most commonly duodenum), creating a cholecystoduodenal fistula; a large (>2.5 cm) gallstone passes through the fistula and impacts in the pylorus or proximal duodenum, obstructing gastric outflow
- Radiograph: May show a markedly distended stomach, pneumobilia (biliary air), and a paucity of distal bowel gas; the classic Rigler triad is rarely all visible on plain film
- CT: Diagnostic gold standard; demonstrates the distended stomach, pneumobilia, the cholecystoduodenal fistula, a thickened gallbladder wall with surrounding inflammation, and a calcified gallstone impacted in the pylorus/proximal duodenum
- Signs: Rigler triad — pneumobilia, small bowel/gastric outlet obstruction, and ectopic gallstone; Bouveret sign refers to the specific duodenal/pyloric impaction of a gallstone via a biliary-enteric fistula
- DDx: Peptic ulcer disease with gastric outlet obstruction (no pneumobilia or fistula); pancreatic head adenocarcinoma (pancreatic mass without pneumobilia); duodenal carcinoma (primary bowel mass, no fistula); classic gallstone ileus (stone typically lodged at the ileocecal valve in the right iliac fossa)
- Tx: Endoscopic retrieval is first-line but often unsuccessful due to large stone size; definitive management requires surgical enterolithotomy or gastrotomy with stone extraction, with single-stage or two-stage cholecystectomy and fistula repair; high morbidity (~30%) due to elderly, comorbid population
OSCE Questions
Question: Name the three components of the classic radiographic triad for this condition.
Pneumobilia, ectopic gallstone, and bowel (gastric/duodenal) obstruction.
Question: What abnormal communication between organs underlies the pathophysiology of this condition?
A biliodigestive (cholecystoenteric) fistula.
Question: What is the first-line cross-sectional imaging modality for this condition?
Contrast-enhanced CT.
Question: What related condition causes obstruction at the ileocecal valve?
Classic (distal) gallstone ileus.
Question: What is the preferred initial intervention for stone removal in this condition?
Endoscopic stone extraction (with or without lithotripsy).
MCQ Questions
1. Which finding completes the classic imaging triad?
A. Ectopic gallstone
B. Portal venous gas
C. Pneumoperitoneum
D. Hepatosplenomegaly
Answer: A. Ectopic gallstone. Rigler’s triad comprises pneumobilia, bowel obstruction, and an ectopic gallstone, all resulting from the underlying biliary-enteric fistula.
2. Where does the obstructing stone typically lodge in this syndrome?
A. Terminal ileum
B. Sigmoid colon
C. Pylorus or duodenum
D. Rectum
Answer: C. Pylorus or duodenum. Bouveret syndrome is defined by proximal impaction at the pylorus or duodenum, distinguishing it from classic gallstone ileus at the terminal ileum.
3. What demographic is most commonly affected by this syndrome?
A. Young males
B. Adolescents
C. Middle-aged males
D. Elderly females
Answer: D. Elderly females. Chronic cholelithiasis and cholecystitis are more prevalent in elderly females, explaining this syndrome’s demographic predilection.
4. What is the underlying cause of this syndrome?
A. Pancreatic pseudocyst
B. Biliary-enteric fistula
C. Intestinal volvulus
D. Mesenteric ischemia
Answer: B. Biliary-enteric fistula. Chronic gallbladder inflammation erodes into the adjacent bowel, creating a fistula that permits gallstone passage into the GI tract.
5. What is the surgical treatment for this syndrome?
A. Enterolithotomy
B. Cholecystectomy alone
C. ERCP with stenting
D. Antibiotics only
Answer: A. Enterolithotomy. Enterolithotomy directly removes the obstructing stone via gastrotomy or enterotomy when endoscopic retrieval fails or is contraindicated.
Check out more such cases:






Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case