
65-year-old male presenting with acute onset dizziness, nausea, and unsteady gait. What is your diagnosis?
Diagnosis and teaching points:
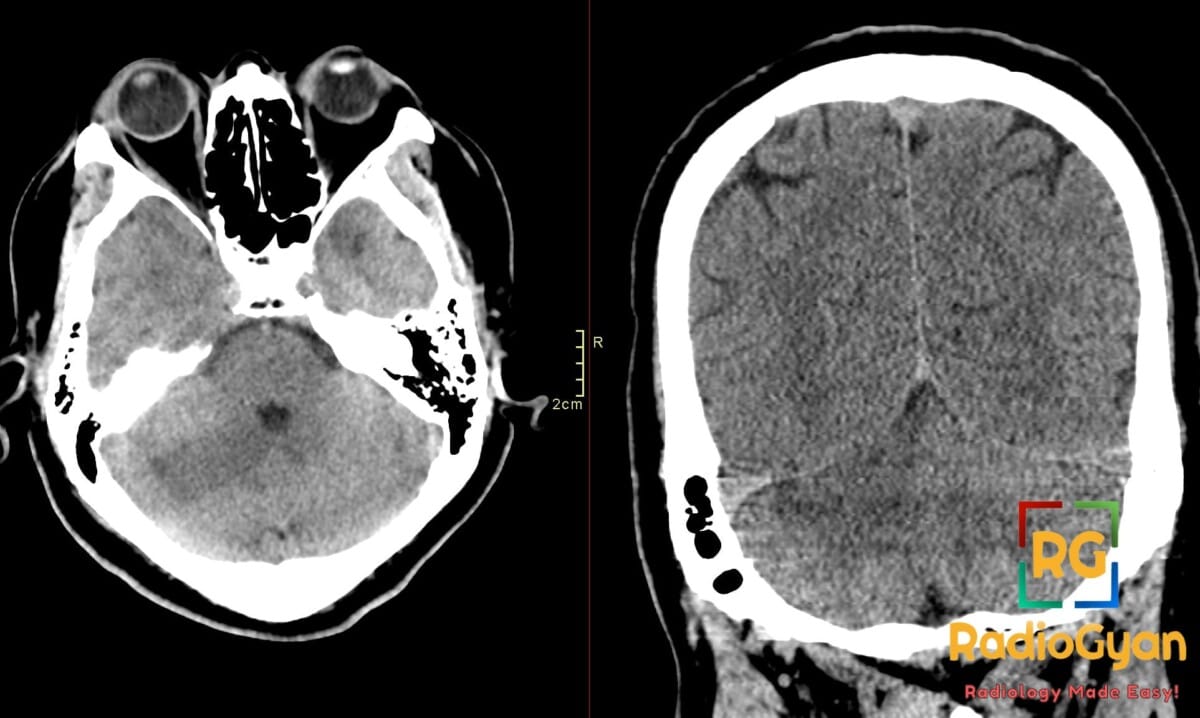
Diagnosis: Right superior cerebellar artery (SCA) territory infarct.
Key facts for board exams:
- Most common cerebellar artery territory infarct, accounting for the largest share of posterior circulation strokes involving the cerebellum.
- Classic triad of ipsilateral ataxia, vertigo/dizziness, and ipsilateral Horner syndrome; headache is common.
- Non-contrast CT is often negative early; MRI with DWI is the most sensitive and specific test for acute infarction.
- Mass-effect risk from cerebellar swelling can cause obstructive hydrocephalus and tonsillar herniation, a neurosurgical emergency.
- Frequently misdiagnosed initially as vestibular neuritis — a key board “do-not-miss” pitfall when the HINTS exam is central.
Detailed teaching points:
- Clinical: Older adults with vascular risk factors (hypertension, atrial fibrillation, diabetes, smoking); presents with vertigo, ipsilateral limb ataxia, dysmetria, gait instability, nausea, and headache.
- Etiology/Pathophys: Embolic occlusion (cardioembolic or artery-to-artery from vertebrobasilar atherosclerosis) of the SCA, which arises from the basilar artery just before its terminal bifurcation and supplies the superior cerebellum, dentate nucleus, and superior cerebellar peduncle.
- CT: Non-contrast CT shows ill-defined hypodensity in the superior/cerebellar hemisphere with loss of gray–white differentiation; hyperdense SCA sign is rarely seen; assess for fourth-ventricular effacement, basal cistern crowding, and obstructive hydrocephalus.
- MRI: DWI is the gold standard showing restricted diffusion within hours; hyperintense on FLAIR/T2 and hypointense on T1 in the SCA territory; contrast-enhanced MRA/CTA can demonstrate the filling defect or absent flow in the SCA.
- US: Transcranial Doppler can demonstrate elevated velocities or absence of flow in the SCA; carotid duplex may identify a proximal embolic source.
- Signs: Hyperdense artery sign (acute thrombus in SCA on CT); disappearing basilar artery sign with occlusion; central HINTS exam (normal head impulse, direction-changing nystagmus, skew deviation) suggests posterior circulation stroke rather than vestibular neuritis.
- Frameworks: ABCD2 score for TIA risk; ASPECTS does not apply to posterior fossa — use pc-ASPECTS for posterior circulation stroke; consider NIHSS (often underestimates severity in cerebellar stroke).
- DDx: Vestibular neuritis (peripheral HINTS, no DWI lesion); PICA infarct (lateral medullary/Wallenburg signs, more lateral inferior cerebellum); AICA infarct (lateral pontine signs + facial nerve involvement); cerebellar hemorrhage (hyperdense on CT, no vascular territory restriction).
- Tx: IV thrombolysis (tPA/tenecteplase) within window; mechanical thrombectomy for large-vessel posterior circulation occlusion; suboccipital decompressive craniectomy for malignant cerebellar edema with brainstem compression/hydrocephalus; secondary prevention with antiplatelet or anticoagulation depending on etiology.
OSCE Questions
Question: What is the most sensitive imaging modality for early detection of this pathology?
DWI-MRI (diffusion-weighted MRI), which detects restricted diffusion within minutes of symptom onset.
Question: What clinical term describes this infarct when massive edema causes brainstem compression?
Malignant cerebellar infarct.
Question: Which cerebellar artery territory infarct is classically differentiated by ipsilateral hearing loss?
AICA (anterior inferior cerebellar artery) infarct, due to internal auditory artery involvement.
Question: What surgical procedure is indicated for malignant edema with impending herniation?
Decompressive suboccipital craniectomy.
Question: What adjacent structure’s compression by edema can mimic a primary brainstem infarct on CT?
The brainstem (pons), due to mass effect from posterior fossa swelling.
MCQ Questions
1. Which modality is gold standard for early posterior fossa ischemia?
A. Non-contrast CT
B. CT angiography
C. MRI with DWI
D. Transcranial Doppler
Answer: C. MRI with DWI. DWI detects cytotoxic edema within minutes, while early posterior fossa ischemia is frequently missed on CT due to beam-hardening artifact.
2. What surgery is indicated for malignant cerebellar edema?
A. Decompressive craniectomy
B. External ventricular drain
C. Carotid endarterectomy
D. Endovascular coiling
Answer: A. Decompressive craniectomy. Massive cerebellar edema causes brainstem compression and herniation, requiring surgical decompression to prevent death.
3. What complication arises from posterior fossa mass effect?
A. Subarachnoid hemorrhage
B. Aneurysm formation
C. Sinus thrombosis
D. Brainstem compression
Answer: D. Brainstem compression. Cytotoxic and vasogenic edema in the tight posterior fossa compresses the brainstem, risking herniation and obstructive hydrocephalus.
4. Which symptom suggests concomitant labyrinthine artery involvement?
A. Anosmia
B. Sensorineural hearing loss
C. Visual field defect
D. Hemiparesis
Answer: B. Sensorineural hearing loss. The labyrinthine (internal auditory) artery typically arises from AICA, so its involvement produces hearing loss/vertigo absent in SCA infarcts.
5. What cerebellar region does this artery supply?
A. Inferior vermis
B. Cerebellar tonsils
C. Superior vermis
D. Middle cerebellar peduncle
Answer: C. Superior vermis. The SCA perfuses the superior vermis and superior cerebellar hemispheric surface, distinguishing it from PICA (inferior) and AICA (anteroinferior) territories.
Check out more such cases:


Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case