
55-year-old female with progressive dyspnea and dry cough. What is your diagnosis?
Diagnosis and teaching points:
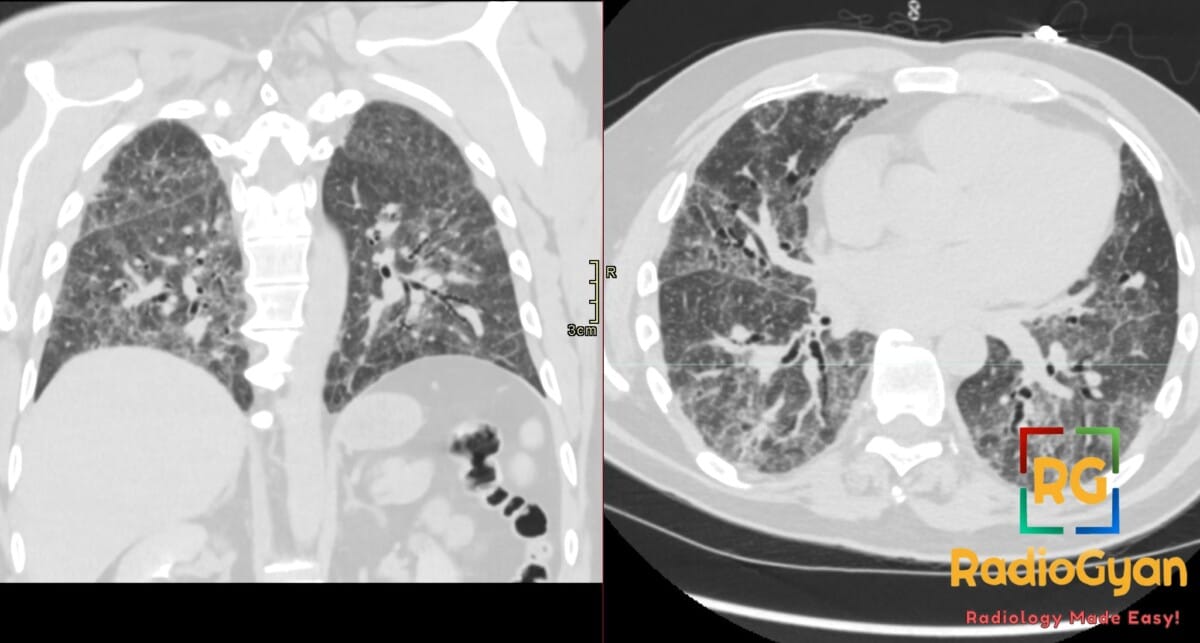
Diagnosis: Fibrotic hypersensitivity pneumonitis. HRCT chest shows reticulation and traction bronchiectasis.
Key facts for board exams:
- Fibrotic HP is characterized on HRCT by reticulation, traction bronchiectasis/bronchiolectasis, and volume loss, often with upper/mid lung predominance.
- The three-density sign (mosaic attenuation with both ground-glass and areas of low attenuation/lobular air-trapping) is highly suggestive of fibrotic HP.
- Centrilobular ground-glass nodules and air-trapping on expiratory imaging are characteristic findings of hypersensitivity pneumonitis.
- Common causative antigens include avian (bird fancier’s), moldy hay (farmer’s lung), and contaminated water/mold exposure; history of exposure is essential for diagnosis.
- Fibrotic HP can mimic idiopathic pulmonary fibrosis (IPF)/UIP; key differentiators are upper-lung predominance, air-trapping, and absence of honeycombing in early disease.
Detailed teaching points:
- Clinical: Typically presents in adults (40–60s); symptoms include progressive dyspnea and dry cough; history of antigen exposure is the key diagnostic clue.
- Etiology/Pathophys: Immune-mediated (type III and IV hypersensitivity) inflammatory response to inhaled organic or low-molecular-weight antigens, progressing to fibrosis with continued exposure.
- CT: HRCT shows reticulation, traction bronchiectasis, and architectural distortion with upper- and mid-zone predominance; mosaic attenuation, lobular air-trapping (best on expiratory imaging), and centrilobular ground-glass nodules; honeycombing may occur in advanced disease but is less extensive than in UIP/IPF.
- Signs: Three-density sign (combination of ground-glass, normal lung, and hyperlucent lobules); mosaic attenuation from small airways disease; headcheese sign refers to the heterogeneous mixture of densities on inspiratory HRCT.
- Frameworks: Diagnostic criteria (CHEST 2020/Jacobs) integrate exposure history, HRCT pattern (typical vs. compatible with HP), and bronchoalveolar lavage lymphocytosis with histopathology when needed.
- DDx: IPF/UIP — basal/subpleural honeycombing, traction bronchiectasis; NSIP — lower-zone ground-glass with subpleural sparing; sarcoidosis — perilymphatic nodules and hilar/mediastinal lymphadenopathy; respiratory bronchiolitis (RB-ILD) — smoking-related upper-zone centrilobular nodules with ground-glass.
- Tx: Antigen avoidance is the cornerstone of management; systemic corticosteroids for acute/symptomatic disease; antifibrotic therapy (e.g., nintedanib) considered in progressive fibrosing disease; pulmonary rehabilitation and lung transplant for advanced fibrosis.
OSCE Questions
Question: What CT sign is relatively specific for this pathology and involves three coexisting lung densities?
The head cheese sign (three-density pattern): ground-glass opacity, lobular air trapping, and normal intervening lung.
Question: What imaging maneuver is essential to demonstrate lobular air trapping in this disease?
Expiratory CT acquisition, since air trapping is often occult on inspiratory scans.
Question: What distribution feature distinguishes this condition from idiopathic pulmonary fibrosis?
Sparing of the lung bases, with fibrosis favoring the mid- and upper-zone peribronchovascular regions.
Question: What is the first-line management for this immune-mediated lung disease?
Identification and removal of the inciting inhaled antigen.
Question: What is the imaging modality of choice for evaluating this interstitial lung disease?
High-resolution CT (HRCT) of the chest.[/spoiler
MCQ Questions
1. Classic CT sign combining ground-glass, normal lung, and air trapping
A. Tree-in-bud pattern
B. Head cheese sign
C. Crazy paving pattern
D. Mosaic attenuation alone
Answer: B. Head cheese sign. This three-density pattern reflects coexistent inflammation (ground-glass), small airway obstruction (air trapping), and spared normal lobules within the same secondary pulmonary lobule.
2. Most common cause of this immune-mediated interstitial disease
A. Autoantibody formation
B. Drug toxicity
C. Inhaled organic antigens
D. Radiation exposure
Answer: C. Inhaled organic antigens. HP is triggered by sensitization to environmental antigens such as bird proteins, molds, and thermophilic bacteria, prompting a hypersensitivity reaction.
3. Which lung zone is characteristically spared in this entity?
A. Upper zones
B. Right middle lobe
C. Lung bases
D. Apical segments
Answer: C. Lung bases. Relative basal sparing is a key discriminator of fibrotic HP from idiopathic pulmonary fibrosis, which is characteristically basal and subpleural predominant.
4. Best CT phase to demonstrate lobular air trapping
A. Expiratory imaging
B. Inspiratory imaging
C. Prone imaging
D. Supine imaging
Answer: A. Expiratory imaging. Air trapping from bronchiolar inflammation is often occult on inspiratory scans, making paired expiratory acquisitions essential to confirm the three-density pattern.
5. This entity is also known as
A. Idiopathic pulmonary fibrosis
B. Cryptogenic organizing pneumonia
C. Extrinsic allergic alveolitis
D. Desquamative interstitial pneumonia
Answer: C. Extrinsic allergic alveolitis. The older term emphasizes the extrinsic antigen trigger and alveolar-centered immune response that defines this hypersensitivity reaction.
Check out more such cases:




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case