
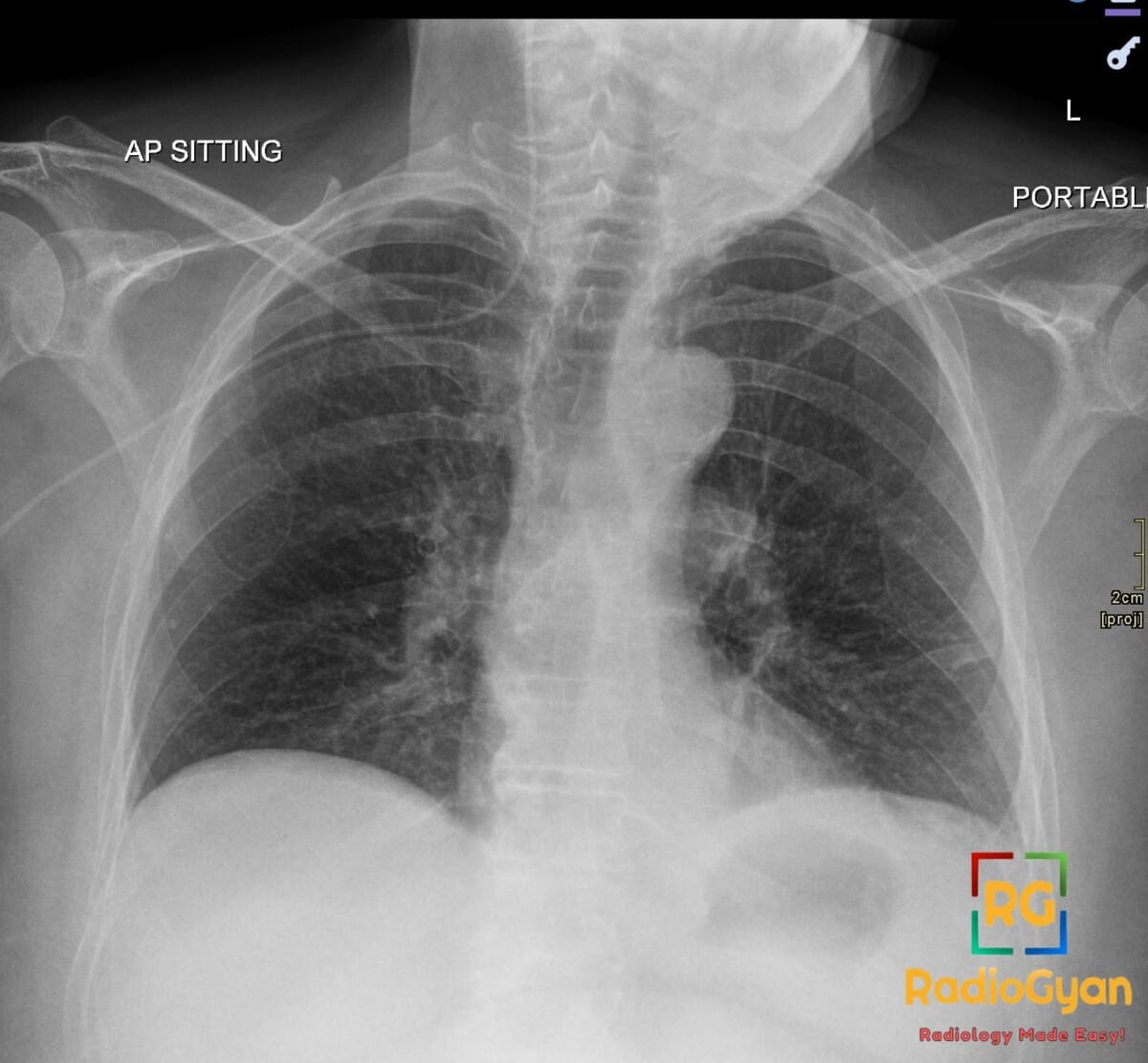
50-year-old female with breast cancer presenting for routine follow-up imaging. What is your diagnosis?
Diagnosis and teaching points:
Diagnosis: PICC line malposition. The catheter tip courses cephalad into the right internal jugular vein on chest radiograph.
Key facts for board exams:
- PICC (peripherally inserted central catheter) tip should sit at the cavoatrial junction / lower SVC for safe use.
- Malposition into the ipsilateral internal jugular vein is a common abnormal course, often from tip redirecting cephalad at the brachiocephalic confluence.
- Always obtain a post-procedure chest radiograph to confirm tip position before infusing vesicants (e.g., vasopressors, TPN, chemotherapy).
- Cephalad-misdirected PICC tips are at risk for venous thrombosis, vessel injury, and inaccurate drug delivery and must be repositioned or removed.
- If the line cannot be easily withdrawn, fluoroscopic or IR-guided repositioning is the next step; CT is reserved for suspected complications (thrombosis, perforation).
Detailed teaching points:
- Clinical: PICCs are placed in upper-arm basilic, brachial, or cephalic veins for long-term IV access in patients needing antibiotics, chemotherapy, TPN, or repeated blood sampling; malposition rates approach 5–10%.
- Etiology/Pathophys: Cephalad tip migration into the internal jugular vein occurs when the catheter preferentially tracks upward at the junction of the subclavian and brachiocephalic veins, often related to arm position, large vein caliber, or short catheter length.
- Radiograph: Tip projects above the level of the clavicular head within the right paratracheal/IJ region rather than at the right paratracheal stripe near the right mainstem bronchus; the catheter courses cranially instead of curving into the SVC.
- US: Bedside vascular ultrasound of the neck confirms the catheter within the IJ lumen and excludes internal jugular vein thrombosis as a complication.
- CT: CT venogram or contrast-enhanced chest CT may be used when radiograph is equivocal or to evaluate for catheter-related thrombosis, mediastinal hematoma, or vessel perforation.
- Signs: “Cephalad loop” sign describes the catheter curving superiorly into the IJ; the tip-above-clavicle sign flags an inappropriately high, non-central position.
- Frameworks: Per INS (Infusion Nurses Society) and ACR guidelines, the acceptable PICC tip position is the lower third of the SVC at the cavoatrial junction; any other location is considered malpositioned and requires correction before use.
- DDx: Other malposition sites include contralateral subclavian/brachiocephalic vein, azygos vein (azygos arch sign), internal mammary vein, contralateral IJ, and right atrium/ventricle (too deep, risk of arrhythmia/perforation).
- Tx: Withdraw the catheter to the correct length and re-image, or have interventional radiology reposition under fluoroscopy; remove the line if it cannot be repositioned safely; obtain a follow-up radiograph to confirm final tip location before use.
OSCE Questions
Question: What imaging modality is the gold standard for confirming catheter tip position?
Anteroposterior (AP) chest radiograph.
Question: What is the correct anatomical target for the catheter tip?
The cavo-atrial junction (CAJ).
Question: Name the malposition in which the catheter courses posteriorly through the azygos arch.
Azygos vein malposition.
Question: What is the first-line corrective maneuver for this malposition?
Repositioning using an angled guidewire under fluoroscopic guidance.
Question: What is the most significant thrombotic complication of leaving the catheter in this position?
Internal jugular vein thrombosis.
MCQ Questions
1. What is the ideal target tip location for this catheter?
A. Aortic arch
B. Cavo-atrial junction
C. Right ventricle
D. Subclavian vein
Answer: B. Cavo-atrial junction. The cavio-atrial junction is the standard target for central venous catheter tips, ensuring rapid dilution of infusates in the high-flow right atrium.
2. Most common site of malposition for this catheter?
A. Renal vein
B. Azygos vein
C. Internal jugular vein
D. Hepatic vein
Answer: C. Internal jugular vein. The IJV accounts for the highest frequency of PICC malposition, occurring when the catheter fails to descend into the SVC and instead courses cephalad.
3. Imaging modality of choice to confirm this malposition?
A. MRI
B. Ultrasound
C. CT angiography
D. Chest radiograph
Answer: D. Chest radiograph. A single AP chest radiograph is the gold standard for confirming tip position, with the carina serving as the key anatomic landmark.
4. Direction of catheter course in this malposition?
A. Cephalad
B. Inferior
C. Lateral
D. Posterior
Answer: A. Cephalad. Malposition is characterized by the catheter tip turning upward (cephalad) from the brachiocephalic vein into the IJV, rather than descending into the SVC.
5. Most concerning vascular complication if this is left uncorrected?
A. Pulmonary embolism
B. Internal jugular thrombosis
C. Aortic dissection
D. Renal vein thrombosis
Answer: B. Internal jugular thrombosis. A malpositioned tip in the IJV irritates the venous wall and can precipitate thrombus formation, in addition to rendering the line non-functional.
Check out more such cases:



Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case