
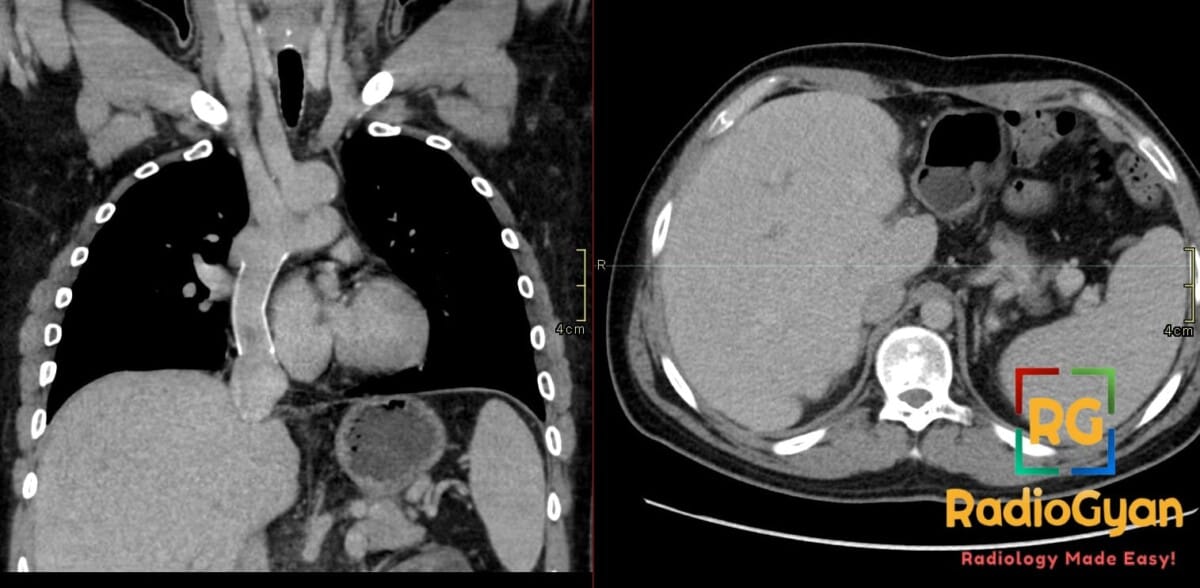
25 yr male with history of congenital heart disease.
Diagnosis and teaching points:
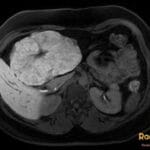
Diagnosis:Cardiac Cirrhosis secondary to Fontan procedure. CT demonstration of cardiac cirrhosis post Fontan procedure.
Key facts for boards exams:
– Fontan-associated liver disease (FALD) ranges from passive congestion to cirrhosis and HCC with many patients clinically silent.
– Occurs years to decades after Fontan surgery due to chronically elevated central venous pressure and reduced hepatic venous pulsatility.
– Imaging shows hepatomegaly, dilated hepatic veins/IVC, heterogeneous reticular enhancement, nodular contour, and signs of portal hypertension.
– Nutmeg liver and mosaic enhancement reflect centrilobular congestion progressing to reverse lobulation fibrosis.
– Surveillance with US/CT/MRI plus elastography is key; optimize Fontan hemodynamics and screen for HCC; liver or combined heart-liver transplant in advanced cases.
Detailed teaching points:
- Clinical: Years to decades after Fontan surgery; no strong sex predilection; often asymptomatic or with ascites splenomegaly varices edema fatigue; risk factors include longer time since Fontan elevated central venous pressure reduced cardiac output Fontan failure; etymology refers to cirrhosis from chronic congestive hepatopathy
- Etiology/Pathophys: Fontan reroutes systemic venous blood to pulmonary arteries causing elevated central venous pressure and reduced pulsatility leading to passive congestion sinusoidal dilatation centrilobular atrophy fibrosis and bridging fibrosis to cirrhosis
- Radiograph: Nonspecific may show cardiomegaly postoperative changes massive ascites or pleural effusions low yield for hepatic disease
- US: Hepatomegaly dilated hepatic veins/IVC coarse heterogeneous nodular echotexture splenomegaly ascites collaterals abnormal Doppler waveforms reduced pulsatility
- CT: Hepatomegaly dilated hepatic veins/IVC heterogeneous reticular zonal enhancement nodular contour surface irregularity splenomegaly ascites portosystemic collaterals hypervascular nodules delayed abnormal enhancement
- MRI: Hepatomegaly heterogeneous congestion fibrotic nodular contour perfusion abnormalities T2 heterogeneity increased stiffness on elastography hypervascular FNH-like nodules
- Nuc Med: No hallmark findings not primary for diagnosis
- Signs: Nutmeg liver mottled appearance from venous congestion; mosaic/reticular enhancement alternating congested regions; cardiac cirrhosis pattern nodular liver with venous congestion in Fontan physiology; reverse lobulation fibrosis linking central veins; hypervascular regenerative/FNH-like nodules from altered perfusion mimicking HCC
- Frameworks: Spectrum from congestive hepatopathy to perisinusoidal fibrosis bridging fibrosis cirrhosis portal hypertension and malignancy; time after Fontan portal hypertension and cross-sectional findings guide monitoring no single imaging-only staging
- DDx: Conventional cirrhosis lacks Fontan link and venous congestion; other congestive hepatopathy from right heart failure tricuspid regurgitation constrictive pericarditis; Budd-Chiari involves thrombosis not Fontan; HCC distinguished by washout capsule growth from benign nodules; FNH-like nodules common in altered perfusion
- Tx: Optimize Fontan hemodynamics surveillance for progression and HCC manage portal hypertension complications liver or combined heart-liver transplant for advanced disease workup suspicious nodules with serial imaging MRI/CT or biopsy
OSCE Questions
Question: What is the best cross-sectional modality for characterization and surveillance of this condition?
MRI with contrast and elastography.
Question: Which sign describes the mottled hepatic appearance from chronic venous congestion in this pathology?
Nutmeg liver.
Question: What is the key hemodynamic driver of this condition in the post-Fontan setting?
Chronically elevated central venous pressure with reduced hepatic venous pulsatility.
Question: Which differential is distinguished from this pathology by hepatic vein or IVC thrombosis?
Budd-Chiari syndrome.
Question: What is the initial treatment priority for this condition?
Optimization of Fontan hemodynamics with surveillance for hepatocellular carcinoma.
MCQ Questions
1. What CT enhancement pattern typifies this pathology?
A. Peripheral nodular enhancement
B. Mosaic reticular pattern
C. Targetoid delayed enhancement
D. Persistent homogeneous enhancement
Answer: B. Mosaic reticular pattern. Chronic venous congestion produces alternating zones of hypo- and hyperenhancement.
2. Which histologic feature defines this pathology?
A. Portal-portal bridging fibrosis
B. Centrilobular sinusoidal fibrosis
C. Bile duct proliferation
D. Lymphocytic interface hepatitis
Answer: B. Centrilobular sinusoidal fibrosis. Elevated venous pressure causes zone-3 congestion progressing to reverse lobulation.
3. What nodules commonly develop in this pathology?
A. Hypovascular cysts
B. Hypervascular FNH-like nodules
C. Calcified granulomas
D. Hypodense metastases
Answer: B. Hypervascular FNH-like nodules. Altered perfusion leads to benign arterialized nodules that mimic HCC.
4. Which finding indicates advanced disease on imaging?
A. Smooth liver contour
B. Nodular surface irregularity
C. Normal hepatic vein caliber
D. Absent collateral vessels
Answer: B. Nodular surface irregularity. Cirrhosis produces surface nodularity together with signs of congestion.
Check out more such cases:





Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case