
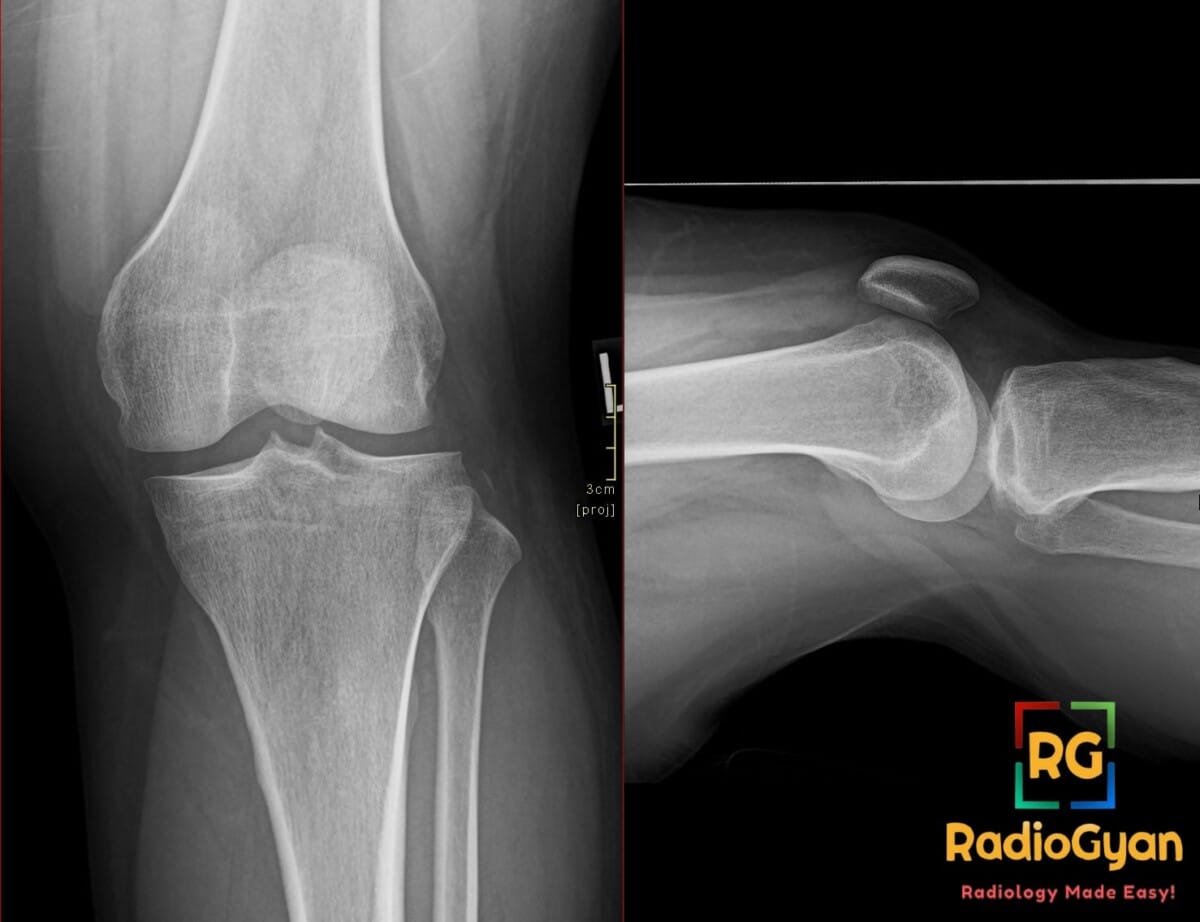
32 yr male presenting with acute knee pain and instability after a high-impact sports injury.
Diagnosis and teaching points:
Diagnosis: Arcuate sign avulsion fracture of the proximal fibula
Key facts for boards exams:
- The arcuate sign is an avulsion fracture of the proximal fibular head styloid process, which serves as an important radiographic marker for posterolateral corner (PLC) injury.
- The avulsed bone fragment is typically small (less than 1 cm), elliptical or fleck-like, horizontally oriented on AP radiographs, and displaced superiorly and medially.
- This injury is highly associated with severe internal derangement of the knee, including ACL tears, PCL tears, and occult knee dislocations.
- It must be distinguished from a Segond fracture, which is an avulsion of the lateral proximal tibia and is strongly associated with anterior cruciate ligament (ACL) tears.
- Identifying an arcuate sign on knee radiographs should immediately prompt an MRI of the knee to fully evaluate the ligaments, menisci, and capsule.
Detailed teaching points:
- Clinical: Occurs in any age group, but typically in young to middle-aged adults with traumatic knee injuries; presents with acute knee pain, swelling, tenderness over the proximal fibula, and potential posterolateral rotatory instability; often accompanies major knee injuries such as ACL, PCL, or posterolateral corner (PLC) injuries; associated with high-energy trauma, varus stress, hyperextension, rotational force, or knee dislocation; named after the arcuate complex of the posterolateral knee.
- Etiology/Pathophys: An avulsion fracture of the fibular head/styloid process at the insertion of the posterolateral corner structures (popliteofibular, arcuate, and fabellofibular ligaments, and occasionally the fibular collateral ligament and biceps femoris tendon); serves as a marker of significant internal derangement (PCL, ACL, and PLC soft-tissue injuries, meniscal tears, and bone bruises); mechanism involves varus stress, external tibial rotation, hyperextension with rotational force, or direct force to the anteromedial knee.
- Radiograph: Shows a small (usually less than 1 cm) elliptical or fleck-like avulsion fragment arising from the proximal fibula/styloid process apex, typically horizontally oriented on the AP view and displaced superiorly and medially; best seen on AP knee radiographs; may be associate with soft tissue swelling and other signs of major knee injury; should prompt evaluation for occult ligamentous injury and potential knee dislocation.
- US: May demonstrate cortical disruption at the proximal fibula, a hypoechoic gap in the bright cortical line at the fibular head, adjacent soft tissue edema, and potential injury of the lateral/posterolateral soft-tissue structures if technically accessible.
- CT: Not routinely required but depicts the tiny avulsion fragment from the fibular head or styloid process with excellent detail, assessing fragment size, displacement, comminution, and any additional occult fractures around the knee.
- MRI: The best diagnostic modality; details the avulsion of the fibular styloid process, injury or discontinuity of the arcuate complex, and tears of posterolateral corner structures (popliteofibular, arcuate, and fibular collateral ligaments, biceps femoris tendon, and posterolateral capsule); assesses associated injuries including classic PCL tears, ACL tears, meniscal tears, signs of posterolateral rotatory instability, and bone bruises (typically located in the anteromedial femoral condyle and anteromedial tibial plateau).
- Signs: The arcuate sign is an avulsion fracture of the fibular head/styloid process representing injury to the posterolateral corner structures; it is distinct from the Segond fracture, which is located more anteriorly/medially on the lateral proximal tibia and is associated with ACL injury.
- Frameworks: There is no formal staging system; the clinical framework categorizes injuries as an isolated arcuate fragment versus a multiligament knee injury; standard practice dictates that finding an arcuate sign on radiograph should prompt an MRI to assess the ligaments, menisci, and bone bruising, and patients should be evaluated for occult knee dislocation within the PLC injury spectrum.
- DDx: Segond fracture (avulsion of the lateral proximal tibia, associated with ACL tear, more medial and anterior than arcuate sign); Fibular head fracture not related to PLC avulsion (often due to direct trauma, more irregular/comminuted, and involves a larger portion of the fibula); Non-ossified soft tissue calcification or old avulsion (chronic, corticated fragment without adjacent marrow edema or acute swelling); Ossicle or accessory ossification center (well-corticated, stable, lacks acute traumatic context); Fabella-related ossification (posterolateral soft tissue ossicle that does not arise from the fibular head); Styloid process fracture from other mechanisms (distinguished by different clinical history and lack of associated PLC ligament injury).
- Tx: Focuses on treating the underlying knee injury rather than the bone fragment alone; immediate priorities include clinical assessment for multiligament and neurovascular injury (if dislocation is suspected) and obtaining an MRI; nonoperative treatment (rest, analgesics, bracing, rehabilitation, and weight-bearing as tolerated) is reserved for truly isolated, stable injuries; operative treatment is indicated for PLC instability, PCL/ACL injuries, knee dislocation, or significant avulsion with joint instability.
OSCE Questions
Question: Injury to which ligamentous complex of the knee is specifically indicated by this radiographic finding?
The posterolateral corner (PLC) or arcuate ligament complex.
Question: Which imaging modality is most appropriate to evaluate for suspected internal derangements associated with this radiographic finding?
Magnetic resonance imaging (MRI).
Question: How is this radiographic finding distinguished from a Segond fracture based on anatomical location?
This condition involves an avulsion of the proximal fibula or fibular styloid, whereas a Segond fracture involves the lateral proximal tibia.
Question: Which cruciate ligament tear is most classically and commonly associated with this injury?
Posterior cruciate ligament (PCL) tear.
Question: The identification of this pathology should prompt immediate clinical and imaging evaluation to rule out which underlying major joint emergency?
Occult or spontaneously reduced knee dislocation.
MCQ Questions
1. What ligament is most classically torn with this fracture?
A. Anterior talofibular ligament
B. Posterior cruciate ligament
C. Deep transverse metatarsal ligament
D. Medial collateral ligament
Answer: B. Posterior cruciate ligament. This avulsion fracture is highly associated with injuries to the posterior cruciate ligament and posterolateral corner structures.
2. Where does this avulsion fracture originate?
A. Lateral tibial plateau
B. Medial femoral condyle
C. Fibular styloid process
D. Gerdy tubercle
Answer: C. Fibular styloid process. This fracture represents an avulsion from the styloid process of the proximal fibula.
3. Which structure attaches to this avulsed fragment?
A. Popliteofibular ligament
B. Patellar tendon
C. Iliotibial band
D. Anterior cruciate ligament
Answer: A. Popliteofibular ligament. The avulsed fragment represents the insertion of the posterolateral corner structures, including the popliteofibular ligament.
4. How is this pathology distinguished from a Segond fracture?
A. It is often larger
B. It arises from the fibula
C. It originates from the tibia
D. It involves the patellar tendon
Answer: B. It arises from the fibula. Unlike a Segond fracture which originates from the lateral tibia, this fracture involves the proximal fibular head.
5. Which physical stress mechanism typically causes this injury?
A. Isolated axial loading
B. Valgus stress with flexion
C. Extreme internal rotation
D. Varus stress and hyperextension
Answer: D. Varus stress and hyperextension. This injury mechanism typically involves varus force, hyperextension, and external tibial rotation.
Check out more such cases:


Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case