
60 yr male presenting with chronic anemia and vague abdominal pain.
Diagnosis and teaching points:
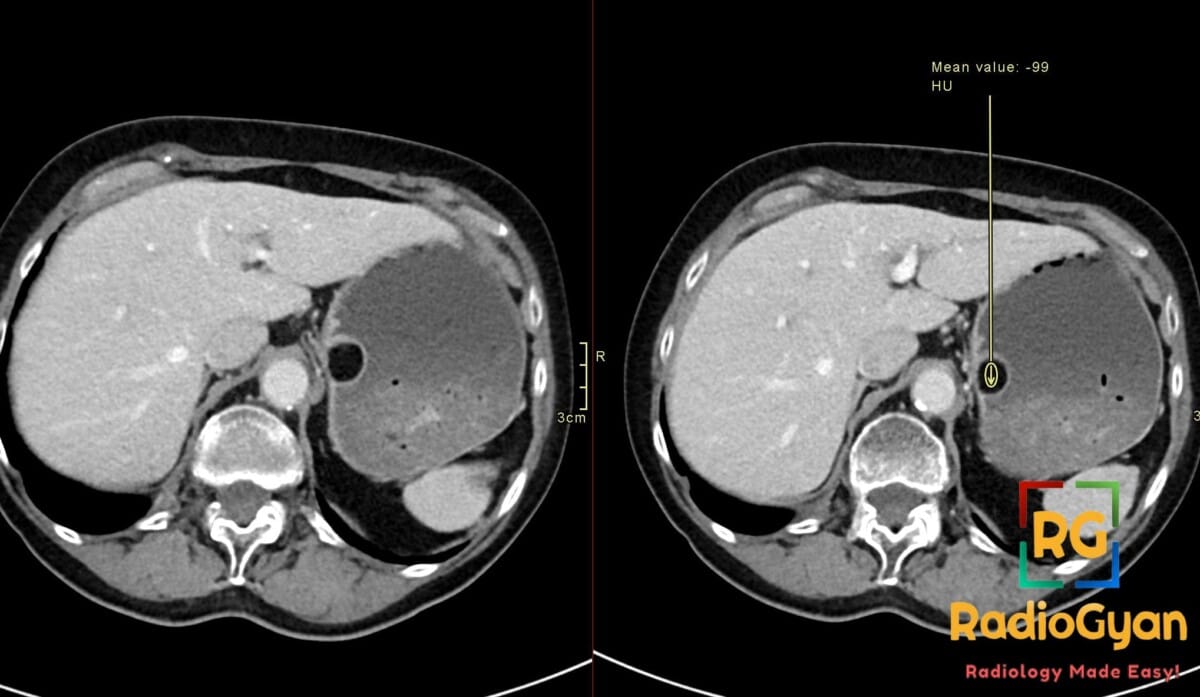
Diagnosis: Gastric lipoma at the fundus
Key facts for boards exams:
- Rare benign mesenchymal tumor accounting for less than 1% of all gastric neoplasms, most commonly found in the antrum.
- Characterized by a pathognomonic homogeneous fat-density appearance on CT with Hounsfield units between -70 and -120.
- Typically asymptomatic when small (<2 cm); lesions larger than 2 cm often present with upper GI bleeding due to overlying mucosal ulceration.
- MRI demonstrates high T1 signal that completely nulls on fat-saturated sequences, confirming the adipose composition.
- Treatment is reserved for symptomatic or large lesions, with endoscopic resection or surgical wedge resection being curative.
Detailed teaching points:
- Clinical: Most common in middle-aged adults; typically asymptomatic if <2 cm; larger lesions cause abdominal pain, dyspepsia, gastric outlet obstruction, or upper GI bleeding (melena, anemia).
- Etiology/Pathophys: Benign tumor of mature adipocytes arising from the gastric submucosa; slow-growing and encapsulated with no malignant potential.
- Radiograph: Upper GI contrast studies may show a smooth filling defect; a central “bulls-eye” sign may be present if the lesion is ulcerated.
- US: Endoscopic ultrasound (EUS) reveals a smooth, hyperechoic submucosal mass.
- CT: Diagnostic modality of choice showing a well-defined, ovoid, homogeneous fat-density mass (-70 to -120 HU) in a submucosal location.
- MRI: Homogeneously hyperintense on T1 and T2 weighted images with complete signal loss on fat-suppression sequences.
- Nuc Med: Not routinely used; typically shows no FDG-PET uptake, which helps exclude malignant gastric tumors.
- Signs: Bulls-eye sign (fluoroscopy): Central ulceration within a filling defect; Fat-density lesion (CT): Homogeneous -70 to -120 HU is pathognomonic.
- DDx: GIST (solid enhancement, FDG-avid, not fat density); Liposarcoma (heterogeneous, larger, possible invasion, higher HU); Leiomyoma (isodense on CT, enhances).
- Tx: Observation for small asymptomatic lesions (<2 cm); endoscopic resection or surgical wedge resection for symptomatic or large (>2 cm) lesions.
OSCE Questions
Question: What is the pathognomonic Hounsfield Unit (HU) range on CT for this condition?
A homogeneous fat-density ranging between -70 to -120 HU.
Question: What is the diagnostic modality of choice for confirming this pathology?
Computed Tomography (CT).
Question: List two common differential diagnosis for this subepithelial gastric mass.
Gastrointestinal stromal tumor (GIST) and leiomyoma.
Question: What is the clinical significance of this lesion reaching a size threshold of greater than 2 cm?
Lesions larger than 2 cm are more likely to become symptomatic, causing obstruction or bleeding from ulceration.
Question: How would this lesion typically behave on fat-saturated MRI sequences?
The signal would suppress completely due to the mature adipocyte content.
MCQ Questions
1. What is the characteristic Hounsfield Unit (HU) range for this gastric lesion?
A. +20 to +50 HU
B. -70 to -120 HU
C. 0 to +10 HU
D. -10 to -30 HU
Answer: B. -70 to -120 HU. This range is pathognomonic for macroscopic fat, confirming the diagnosis of a lipoma.
2. Which imaging sign is associated with this pathology on barium fluoroscopy?
A. Apple core sign
B. Bulls-eye sign
C. Bird beak sign
D. Double bubble sign
Answer: B. Bulls-eye sign. This appearance occurs when central ulceration develops over the submucosal fatty mass.
3. What is the most common gastric location for this benign tumor?
A. Gastric fundus
B. Gastric body
C. Gastric antrum
D. Lesser curvature
Answer: C. Gastric antrum. While it can occur anywhere, the antrum is the most frequent site for gastric lipomas.
4. At what size threshold do these lesions typically become symptomatic?
A. >0.5 cm
B. >1.0 cm
C. >2.0 cm
D. >5.0 cm
Answer: C. >2.0 cm. Lesions smaller than 2 cm are usually asymptomatic, whereas larger ones cause pain or bleeding.
5. Which feature distinguishes this lesion from a GIST on CT?
A. Submucosal origin
B. Homogeneous fat density
C. Size over 3 cm
D. Contrast enhancement
Answer: B. Homogeneous fat density. GISTs are solid and enhancing, while lipomas show characteristic fat attenuation without enhancement.
Check out more such cases:



Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case