
| Cat. | Stenosis | Meaning | Stable / non-acute | Acute chest pain |
|---|---|---|---|---|
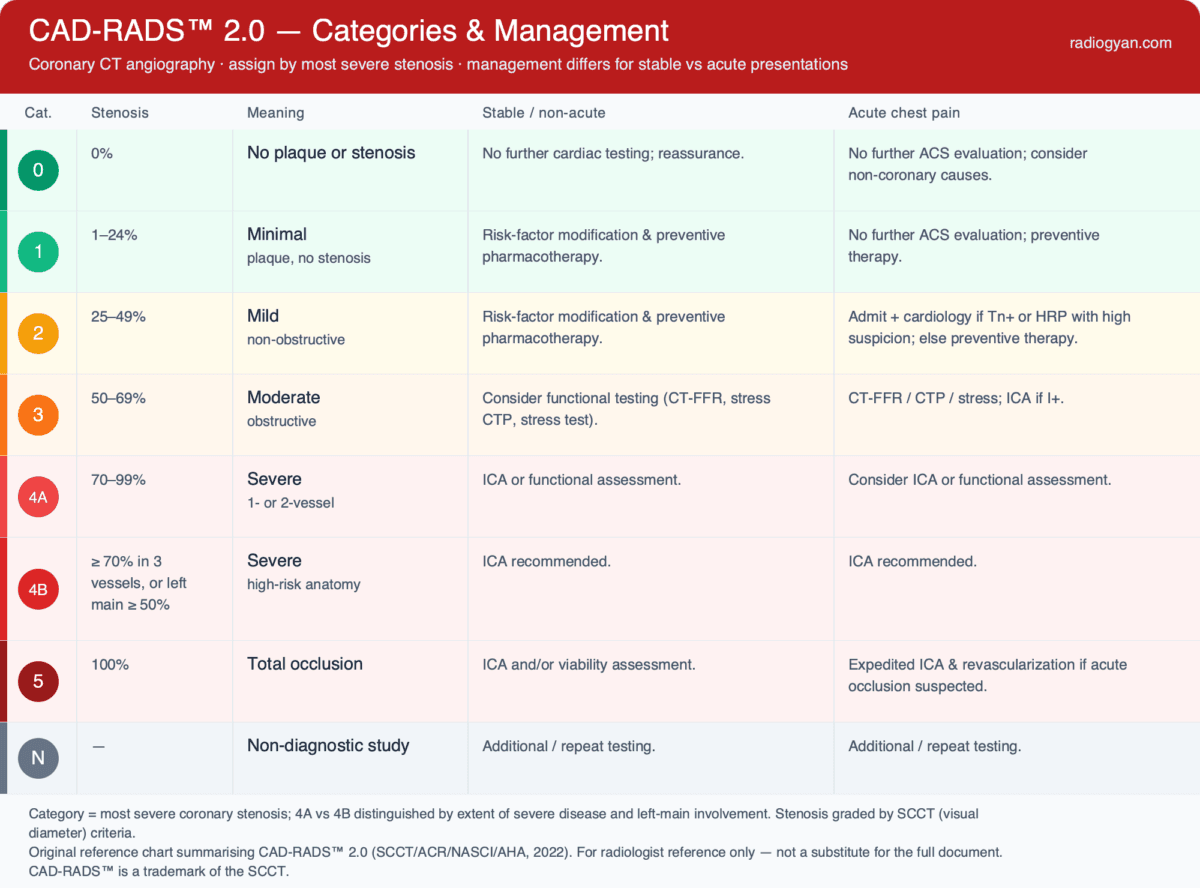
| 0 | 0% | No plaque or stenosis | No further cardiac testing; reassurance | No further ACS evaluation; consider non-coronary causes |
| 1 | 1–24% | Minimal (or plaque, no stenosis) | Risk-factor modification & preventive pharmacotherapy | No further ACS evaluation; preventive therapy |
| 2 | 25–49% | Mild — non-obstructive | Risk-factor modification & preventive pharmacotherapy | Admit + cardiology if Tn+ or HRP & high suspicion; else preventive therapy |
| 3 | 50–69% | Moderate — obstructive | Consider functional testing (CT-FFR, stress CTP, stress test) + preventive therapy | CT-FFR / CTP / stress; ICA if I+ |
| 4A | 70–99% | Severe, 1- or 2-vessel | ICA or functional assessment (CT-FFR / CTP / stress) | Consider ICA or functional assessment |
| 4B | ≥ 70% ×3, or LM ≥ 50% | Severe, high-risk anatomy | ICA recommended | ICA recommended |
| 5 | 100% | Total occlusion | ICA and/or viability assessment | Expedited ICA & revascularization if acute occlusion suspected |
| N | — | Non-diagnostic | Additional / repeat testing | Additional / repeat testing |
| Plaque burden | CAC (Agatston) | SIS |
|---|---|---|
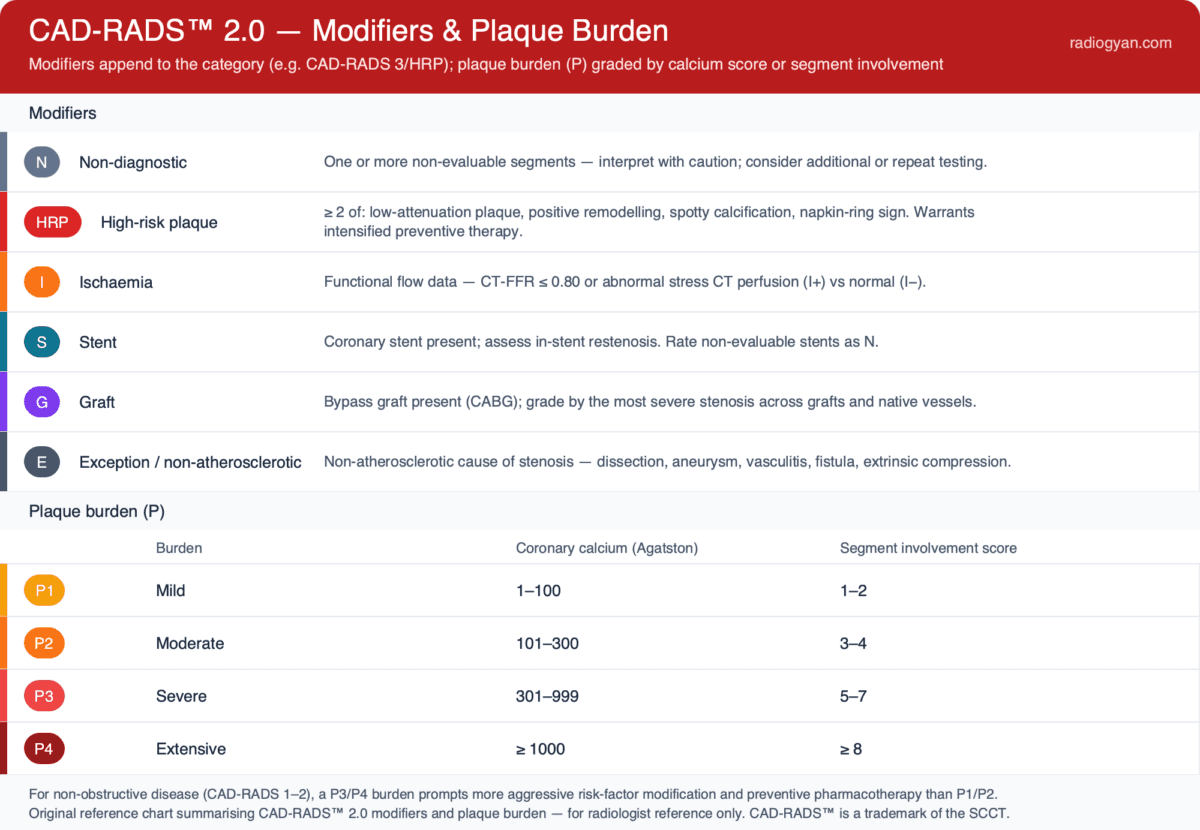
| P1 — mild | 1–100 | 1–2 |
| P2 — moderate | 101–300 | 3–4 |
| P3 — severe | 301–999 | 5–7 |
| P4 — extensive | ≥ 1000 | ≥ 8 |
This tool implements CAD-RADS™ 2.0 (2022, SCCT/ACC/ACR/NASCI). Final classification and management must be made by a qualified physician using the full study and clinical context, including the patient’s presentation (stable vs acute chest pain).
CAD-RADS™ 2.0 Calculator for Coronary CT Angiography
This CAD-RADS calculator assigns the correct Coronary Artery Disease – Reporting and Data System version 2.0 category to a coronary CT angiography (CCTA) study and generates an editable, dictation-ready report. Enter the maximal coronary stenosis, the extent of severe disease, the plaque burden, and any modifiers, and the tool returns the CAD-RADS category, whether the disease is obstructive, and the guideline management recommendation.
Version 2.0, published in 2022, is the current edition. It formalises plaque-burden reporting (P1–P4), renames vulnerable plaque as high-risk plaque (HRP), adds an ischemia modifier for CT-FFR and stress CT perfusion, and splits severe disease into 4A and 4B. The calculator implements these rules and produces report text you can paste into PowerScribe, RadAI or any reporting system.
When CAD-RADS Applies
CAD-RADS 2.0 is intended for the interpretation of coronary CT angiography performed for the evaluation of coronary artery disease in patients with stable or acute chest pain. It is not applied to non-contrast calcium-score-only studies, and it does not replace clinical risk assessment. Every coronary segment with a diameter ≥ 1.5 mm is assessed, and the overall category is driven by the single most severe stenosis regardless of its location. Management recommendations differ between stable and acute presentations; this calculator implements both pathways — select the clinical context (stable / non-acute or acute chest pain, with troponin status) and the recommendation updates accordingly.
How to Use This CAD-RADS Calculator
- Set the clinical context – stable / non-acute or acute chest pain (with troponin status), so the management recommendation follows the correct CAD-RADS 2.0 pathway.
- Select the maximal stenosis – the most severe luminal narrowing in any vessel ≥ 1.5 mm, since the exam is coded by its most significant lesion.
- Define the extent – for severe (70–99%) disease, indicate whether one or two vessels (4A) or all three vessels (4B) are involved, and flag any left main stenosis ≥ 50% (4B).
- Enter the plaque burden – a coronary calcium (Agatston) score, a segment involvement score, or a visual P1–P4 grade; the modifier is derived automatically.
- Add any modifiers – high-risk plaque (HRP), ischemia (I+/I−/I±), stent (S), graft (G), exceptions (E), and non-diagnostic segments (N).
The category, obstructive status and management recommendation update automatically as you complete each field, and a copyable report block appears in the standard CAD-RADS X/Pn/modifiers format.
Categories, Stenosis and Management
| Category | Stenosis | Meaning | Stable / non-acute | Acute chest pain |
|---|---|---|---|---|
| 0 | 0% | No plaque or stenosis | No further cardiac testing; reassurance | No further ACS evaluation; consider non-coronary causes |
| 1 | 1–24% | Minimal (or plaque, no stenosis) | Risk-factor modification & preventive pharmacotherapy | No further ACS evaluation; preventive therapy |
| 2 | 25–49% | Mild — non-obstructive | Risk-factor modification & preventive pharmacotherapy | Admit + cardiology if Tn+ or HRP with high suspicion; else preventive therapy |
| 3 | 50–69% | Moderate — obstructive | Consider functional testing (CT-FFR, stress CTP, stress test) | CT-FFR / CTP / stress; ICA if I+ |
| 4A | 70–99% | Severe, 1- or 2-vessel | ICA or functional assessment | Consider ICA or functional assessment |
| 4B | ≥ 70% in 3 vessels, or left main ≥ 50% | Severe, high-risk anatomy | ICA recommended | ICA recommended |
| 5 | 100% | Total occlusion | ICA and/or viability assessment | Expedited ICA & revascularization if acute occlusion suspected |
| N | — | Non-diagnostic study | Additional / repeat testing | Additional / repeat testing |
Plaque Burden (P1–P4)
A major addition in version 2.0 is the explicit reporting of total plaque burden as a modifier from P1 (mild) to P4 (extensive). Plaque burden may be graded from the coronary artery calcium (CAC) Agatston score, from the segment involvement score (SIS) — the number of coronary segments containing any plaque — or by visual assessment. Because CAC quantifies only calcified plaque, it should be combined with a qualitative assessment of non-calcified plaque when relevant.
| Plaque burden | CAC (Agatston) | Segment involvement score |
|---|---|---|
| P1 — mild | 1–100 | 1–2 |
| P2 — moderate | 101–300 | 3–4 |
| P3 — severe | 301–999 | 5–7 |
| P4 — extensive | ≥ 1000 | ≥ 8 |
The CAD-RADS 2.0 Modifiers
- N (non-diagnostic): not all segments > 1.5 mm are interpretable (e.g. motion artifact, calcium blooming, poor opacification). If an obstructive lesion is still gradeable, score it and append N; otherwise the whole study is CAD-RADS N.
- HRP (high-risk plaque): replaces the term “vulnerable plaque.” Applied when two or more of low-attenuation plaque, positive remodeling, spotty calcification, or the napkin-ring sign are present in the same plaque.
- I (ischemia): indicates dedicated functional testing with CT-FFR or stress CT perfusion. I+ denotes a hemodynamically significant result, I− a negative test or fixed defect / prior infarct, and I± an indeterminate or discrepant result. It is not assigned from the routine CTA appearance alone.
- S (stent) and G (graft): flag the presence of a coronary stent or bypass graft. Native coronary stenoses that are bypassed by a patent graft are not counted toward the CAD-RADS category.
- E (exceptions): non-atherosclerotic causes of coronary narrowing — anomalous origin, dissection, aneurysm or pseudoaneurysm, vasculitis, fistula, or extrinsic compression — which follow disease-specific management.
Modifiers are reported after the category and plaque burden, for example CAD-RADS 4A/P3/HRP/I+. Plaque burden (P) is listed first, followed by N, HRP, I, S, G and E as applicable.
What’s New in CAD-RADS 2.0
- Plaque burden modifier (P1–P4) is now reported routinely, from CAC, SIS or visual assessment, and influences preventive management for non-obstructive disease.
- 4A vs 4B split: severe (70–99%) disease is 4A for one or two vessels and 4B for three-vessel disease or any left main stenosis ≥ 50%.
- High-risk plaque (HRP) replaces “vulnerable plaque,” with the same two-feature definition.
- Ischemia modifier (I) incorporates CT-FFR and stress CT perfusion results as I+, I− or I±.
- Management recommendations were refined, including more aggressive prevention for P3/P4 non-obstructive disease.
Reporting Tips and Common Pitfalls
- Code the exam by the most severe stenosis in any segment ≥ 1.5 mm; the location of that lesion does not change the category.
- Remember that a left main stenosis ≥ 50% is CAD-RADS 4B even when the maximal narrowing elsewhere is only moderate.
- Reserve the I modifier for actual CT-FFR or stress-perfusion results — do not infer ischemia from the anatomic appearance.
- Do not count a native stenosis that is bypassed by a patent graft; grade the grafts and the remaining native vessels instead.
- Always include the plaque-burden modifier, as it carries independent prognostic and preventive-therapy implications even when stenosis is minimal.
Frequently Asked Questions
What is the difference between CAD-RADS 4A and 4B?
Both describe severe (70–99%) stenosis. 4A is single- or two-vessel severe disease, managed with invasive coronary angiography or functional assessment. 4B is reserved for three-vessel severe disease or any left main stenosis ≥ 50% and prompts invasive coronary angiography because of the higher-risk anatomy.
Which stenosis determines the CAD-RADS category?
The single most severe stenosis in any assessable coronary segment determines the category, irrespective of which vessel it is in. The plaque-burden modifier and the other modifiers are reported alongside it.
How is plaque burden graded when only a calcium score is available?
The Agatston coronary calcium score maps to P1 (1–100), P2 (101–300), P3 (301–999) and P4 (≥ 1000). Because the calcium score does not capture non-calcified plaque, the visual or segment-based assessment should be used when significant soft plaque is present.
What does the HRP modifier mean in CAD-RADS 2.0?
HRP (high-risk plaque) replaces the term “vulnerable plaque” and is applied when two or more of low-attenuation plaque, positive remodeling, spotty calcification, or the napkin-ring sign are present in the same plaque. It carries adverse prognostic weight independent of stenosis severity and, in acute chest pain, can escalate management of an otherwise non-obstructive (CAD-RADS 1–2) study.
References
- Cury RC, Leipsic J, Abbara S, et al. CAD-RADS™ 2.0 – 2022 Coronary Artery Disease – Reporting and Data System: An Expert Consensus Document of the SCCT, ACC, ACR and NASCI. JACC: Cardiovascular Imaging. 2022;15(11):1974–2001.
- Cury RC, Leipsic J, Abbara S, et al. CAD-RADS™ 2.0 – 2022 Coronary Artery Disease-Reporting and Data System. Journal of Cardiovascular Computed Tomography. 2022;16(6):536–557.
- Cury RC, Leipsic J, Abbara S, et al. CAD-RADS™ 2.0 – 2022 Coronary Artery Disease – Reporting and Data System. Radiology: Cardiothoracic Imaging. 2022;4(5):e220183.
- Abdelrahman KM, Shah NS, Andrews JD, et al. RadioGraphics Update: Pictorial Guide to CAD-RADS 2.0. RadioGraphics. 2022.
- Cury RC, Abbara S, Achenbach S, et al. CAD-RADS: Coronary Artery Disease – Reporting and Data System (original 2016 consensus). Journal of the American College of Radiology. 2016;13(12):1458–1466.
This calculator implements CAD-RADS™ 2.0 as published in 2022; in case of any discrepancy, the official CAD-RADS 2.0 documents take precedence.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
About the Author
Dr. Amar Udare, MD, DNB
Dr. Udare holds an MBBS and MD degree, and his expertise lies in the field of radiology. He has authored multiple peer-reviewed publications, contributing significantly to the medical field. His works can be accessed on PubMed and Google Scholar.
In addition to his academic and professional achievements, Dr. Udare is an avid reader and enjoys exploring the latest advancements in medical technology. His commitment to making complex medical knowledge accessible to patients and the general public aligns with our mission at RadioGyan.com.
For any further questions or clarifications, feel free to reach out to Dr. Udare via the contact form.