
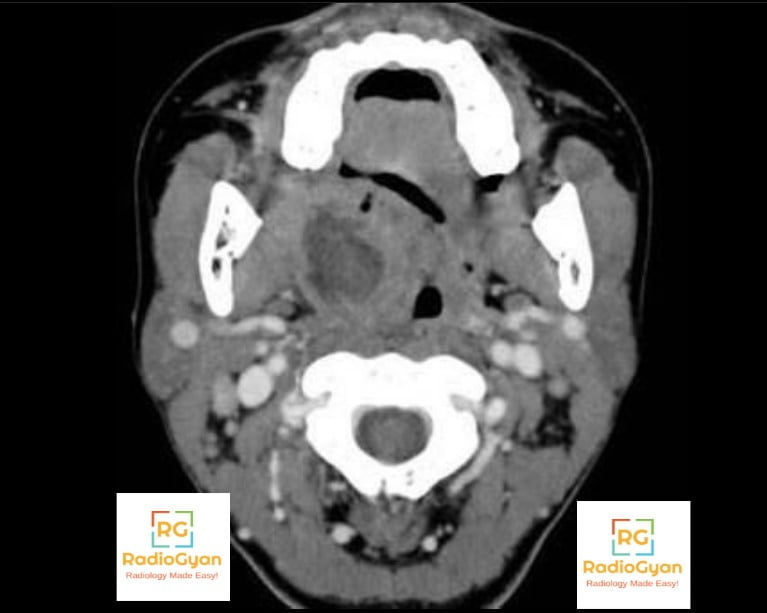
A peritonsillar abscess (PTA) and an intratonsillar abscess (ITA) can both present as a rim-enhancing fluid collection in the tonsillar region on CECT or MRI, but the distinction turns on the collection’s relationship to the fibrous tonsillar capsule. A PTA is extracapsular — it develops in the peritonsillar space, strips the tonsil away from the pharyngeal wall, and displaces it medially. An ITA is intracapsular — it is a purely parenchymal collection completely encircled by tonsillar tissue, with the peritonsillar fat plane left untouched.
The most useful imaging differences are:
| Feature | Peritonsillar Abscess (PTA) | Intratonsillar Abscess (ITA) |
|---|---|---|
| Compartment | Extracapsular — the loose areolar peritonsillar space, between the tonsillar capsule and the superior pharyngeal constrictor. | Intracapsular — entirely within the tonsillar parenchyma, usually from an obstructed crypt. |
| Relationship to tonsil | Separates the tonsil from the pharyngeal wall; appears lateral/superomedial to tonsillar tissue. | Completely enclosed — the rim-enhancing collection is encircled by hyperemic tonsil on all sides. |
| Mass effect / uvula | Marked; pushes the tonsil inferomedially and deviates the uvula to the contralateral side. | Focal, asymmetric tonsillar expansion only; contralateral uvular deviation is rare. |
| Soft palate | Frequently expanded/involved. | Minimal to none. |
| Peritonsillar fat plane | Obliterated or displaced laterally. | Preserved — a clean fat plane argues strongly against PTA. |
| Deep neck space extension | Can breach the superior constrictor to involve the parapharyngeal or masticator space. | Exceptionally rare; extension beyond the tonsil is not expected. |
| Enhancement pattern | Peripherally enhancing collection outside the tonsillar outline. | Rim enhancement fully within the tonsillar outline. |
| How common | The most common deep neck space infection and the most frequent head and neck abscess overall. | Rare in comparison — an uncommon cause of tonsillitis that fails to settle. |
| Typical age | Adolescents and young adults; most series peak in the 20s–40s. | Reported disproportionately more often in children and younger patients than PTA. |
| Trismus | Common and often pronounced — pus tracking laterally irritates the medial pterygoid. | Uncommon or mild — the collection stays confined within the tonsil, sparing the pterygoids. |
| Voice change | Muffled “hot potato” voice is frequent. | Usually normal or only mildly muffled. |
| Drooling | Common, driven by severe odynophagia. | Less common. |
| Referred otalgia | Frequent, via the glossopharyngeal nerve. | Can occur but is less prominent. |
| Cervical lymphadenopathy | Common, tender ipsilateral nodes. | Can be present; less specific for localizing the collection. |
A practical radiology approach is:
- Think PTA when the fat plane lateral to the tonsil is obliterated, the tonsil is pushed medially, and the uvula deviates contralaterally — this is the collection accessible by standard transoral needle aspiration/incision.
- Think ITA when the rim-enhancing collection is fully surrounded by tonsil, the peritonsillar fat plane is clean, and there is little to no uvular shift — this collection sits deep to the standard PTA drainage route and may need image-guided or intracapsular drainage rather than blind needle aspiration.
- Use trismus as a bedside clue that tracks the imaging finding: a patient being treated for “tonsillitis” who fails antibiotics but has no trismus and a normal voice should raise suspicion for an intratonsillar rather than peritonsillar collection.
- Don’t call either one an abscess without a discernible rim. Streaky, parallel hypodense enhancement without a focal fluid collection is cellulitis, not a drainable abscess, and changes management from surgical to medical.
The compartment — not the presence of rim enhancement alone — is what separates these two entities, since both can look identical on a single non-localizing axial slice. Confirming an intact peritonsillar fat plane and lack of uvular deviation is what should push the read toward ITA over the far more common PTA, because it changes the surgical approach ENT will take to drain it.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case