

Key facts for practice and radiology board exams
Aortic dissection is an intimal tear that lets blood into the media and splits it longitudinally into a true and a false lumen. It is one of three acute aortic syndromes, alongside intramural hematoma (IMH) and penetrating atherosclerotic ulcer (PAU). Only one question drives immediate management: is the ascending aorta involved? If yes, it is Stanford type A — a surgical emergency carrying roughly 1%–2% mortality per hour while untreated. If no, it is type B, managed medically with anti-impulse therapy unless complicated, in which case TEVAR is the preferred intervention. ECG-gated CT angiography from thoracic inlet to femoral heads, with a preceding non-contrast series, is the imaging workhorse.[1][2][3]
Quiz
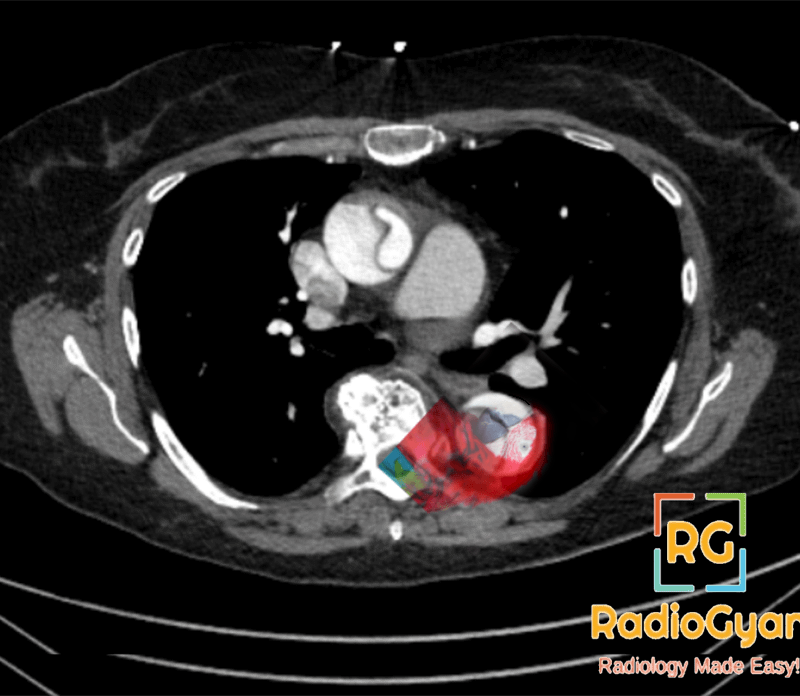
Identify the type of aortic dissection in the CT above.
- Stanford Type A
- Stanford Type B
- Stanford Type C
The three acute aortic syndromes
Dissection is the prototype, but clinical presentation cannot separate the three entities — imaging does.[3] All three are stratified by the same Stanford A/B rule and carry the same urgency when the ascending aorta is involved.
| Entity | Defining CT finding | Key point |
|---|---|---|
| Aortic dissection | Intimal flap separating two contrast-opacified lumens | Entry tear location and ascending involvement drive management |
| Intramural hematoma (IMH) | Crescentic high-attenuation (≈60–70 HU) wall thickening >5 mm on non-contrast CT, no flap, no enhancement | Missed if a non-contrast series is not acquired; may progress to overt dissection or regress |
| Penetrating atherosclerotic ulcer (PAU) | Focal contrast outpouching beyond the expected aortic contour through the intima into the media, with adjacent heavy atherosclerosis | Typically descending aorta in older, atherosclerotic patients; may be associated with focal IMH |
IMH deserves specific attention because it is the entity most often under-called. Unlike a dissection flap, IMH maintains a constant circumferential relationship with the aortic wall and does not spiral along the aorta. Features that predict progression to dissection, rupture, or the need for intervention include maximum aortic diameter, hematoma thickness (roughly >10–11 mm), ulcer-like projections, and pericardial or pleural effusion — these should be stated explicitly in the report.[4]
CT protocol for suspected acute aortic syndrome
CT angiography, MR angiography, and transoesophageal echocardiography are all rated usually appropriate for initial evaluation, but CTA is the practical first-line test in almost every emergency department.[2] Three protocol decisions matter:
- Non-contrast series first. This is the only sequence that reliably shows a hyperattenuating crescent of IMH. Skipping it is the single commonest protocol error, because after contrast the hematoma becomes iso- to hypoattenuating relative to the opacified lumen.
- ECG gating for the thorax. Cardiac motion at the aortic root produces a curvilinear pulsation artifact that mimics a flap, classically at the sinotubular junction. Gating removes it and is also what allows confident assessment of the aortic root, coronary ostia, and aortic valve.
- Cover thoracic inlet to femoral heads. Dissection extent, branch vessel involvement, and access vessels for endovascular repair all need to be documented. Truncating at the diaphragm loses the malperfusion assessment that determines whether a type B dissection is complicated.
On radiographs, a widened superior mediastinum (>8 cm) or progressive aortic enlargement is suggestive but neither sensitive nor specific — a normal chest radiograph never excludes dissection. D-dimer is useful as a rule-out adjunct within validated risk-score pathways, not as a standalone test.[5]
True versus false lumen
Correctly labelling the lumens is not academic: endovascular wires and stent-grafts must be delivered into the true lumen, and the false lumen is where aneurysmal degeneration occurs on follow-up.
| True lumen | False lumen | |
|---|---|---|
| Size | Usually smaller, compressed | Usually larger (higher pressure, lower resistance) |
| Shape | Round | Crescentic, wraps around the true lumen |
| Contrast density | Similar to other arteries; opacifies early | Less dense, delayed opacification |
| Thrombosis | Uncommon | Common |
| Continuity | Continuous with undissected aorta | Ends blindly or re-enters distally |
| Specific signs | None | Beak sign, cobweb sign |
Beak sign — the acute angle formed where the false lumen wedges into the aortic wall. It is the most reliable single discriminator.
Cobweb sign — thin, linear strands of incompletely sheared media crossing the false lumen. Specific but seen less often.
Mercedes-Benz sign — a triple-channel appearance produced by a secondary dissection within one of the lumens.
Classification systems
Ascending aorta: Stanford A — Acute worrisome — Acute management (surgical).
Beyond the ascending aorta: Stanford B — Be calm (medical management first).
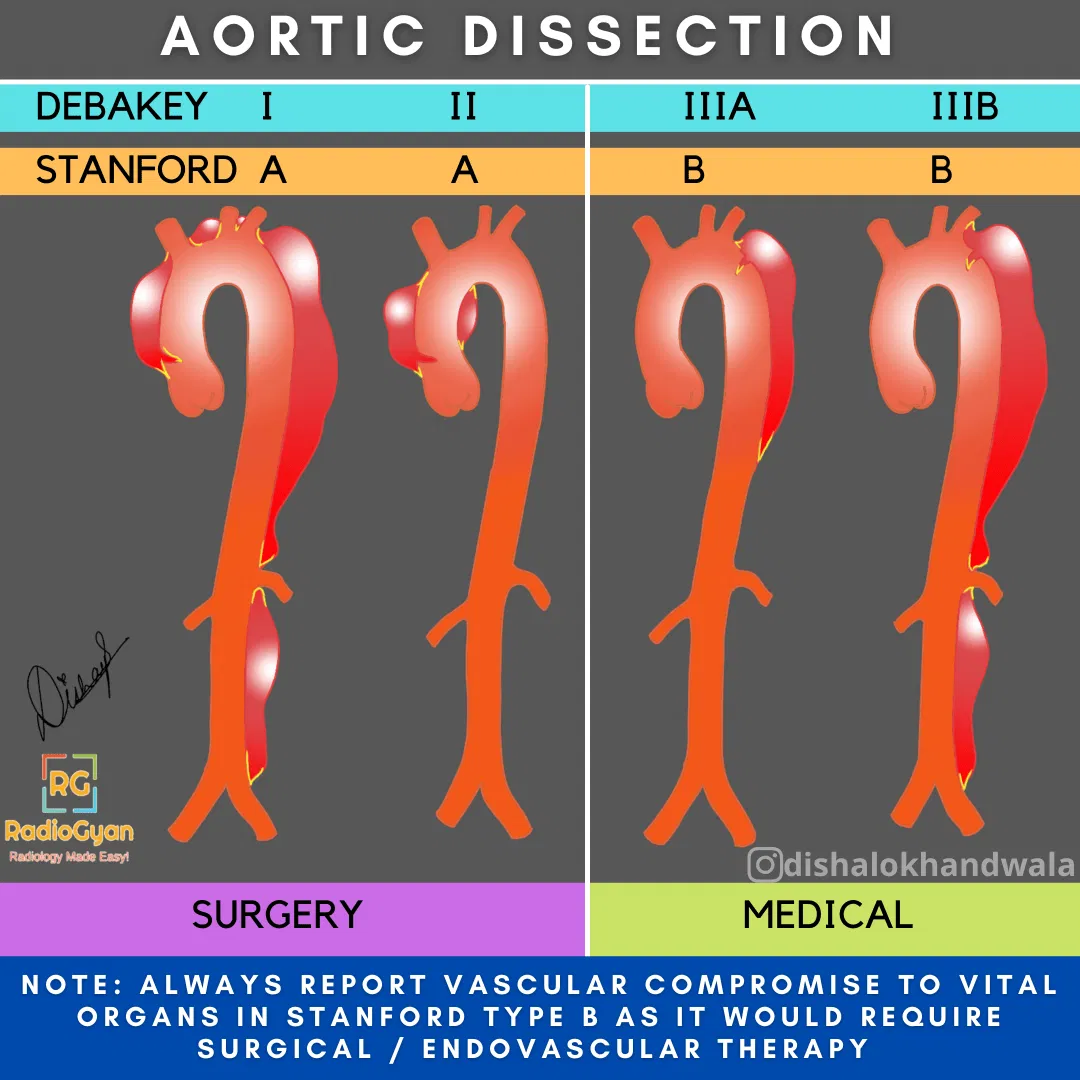
Stanford classification
Type A (≈60%): involves the ascending aorta, regardless of the site of the entry tear.
Type B (≈40%): does not involve the ascending aorta.
DeBakey classification
Type I: originates in the ascending aorta, involves at least the arch, and may extend into the descending aorta.
Type II: originates in and is confined to the ascending aorta.
Type III: originates in the descending aorta; IIIa limited to the descending thoracic aorta, IIIb extends below the diaphragm.
The 2022 ACC/AHA guideline additionally asks for the disease to be timed and for the anatomy to be described beyond the A/B label — specifically the location of the primary entry tear and the proximal and distal extent of the dissected segment, since these determine endovascular planning.[1]
| Phase | Time from symptom onset |
|---|---|
| Hyperacute | < 24 hours |
| Acute | 1–14 days |
| Subacute | 15–90 days |
| Chronic | > 90 days |
Complications to look for
Complications, not the flap itself, decide whether a type B dissection goes to theatre. Malperfusion is the one most often missed, and the mechanism should be specified because it changes the treatment:
- Dynamic malperfusion (more common): the mobile flap prolapses across a branch origin like a curtain, intermittently obstructing it. The branch itself is not dissected. Usually relieved by restoring true lumen flow — TEVAR over the entry tear.
- Static malperfusion: the flap extends into the branch ostium itself, with a fixed narrowing. Often needs branch stenting.
- Type A specific: aortic regurgitation, coronary ostial involvement (right coronary artery most often), haemopericardium and tamponade, and extension into the arch vessels causing stroke.
- Rupture: periaortic or mediastinal haematoma, high-attenuation pleural or pericardial fluid, and active contrast extravasation.
- Organ ischaemia: hypoenhancing kidney, spleen or bowel wall, and asymmetric limb vessel opacification.
Mimics of a dissection flap
False positives carry real consequences — an unnecessary sternotomy call at 3 a.m. Before committing, exclude:
- Pulsation artifact at the aortic root and sinotubular junction. It typically crosses the aortic wall, is not reproducible on a gated series, and does not extend over multiple contiguous slices in a spiralling fashion.
- Streak and beam-hardening artifact from dense contrast in the superior vena cava or left brachiocephalic vein — a common source of a spurious ascending aortic “flap”.
- Periaortic structures: the left superior intercostal vein (aortic nipple), pericardial recesses, thymic tissue, and adjacent atelectasis abutting the aorta.
- Mural thrombus in an aneurysm, which has an irregular inner margin, no beak sign, and no separate opacified lumen.
Reporting checklist
A structured algorithm for reporting CT of the whole aorta, using the mnemonic DISSECTION:[3]
Dissection or other acute aortic syndrome — present or absent?
Is the ascending aorta involved?
Intimal (entry) tear location
Size of the true and false lumens
Segments of aorta involved, and proximal/distal extent
Extent of aortic branch involvement
Complications — rupture, malperfusion, tamponade
Thrombus in the false lumen, and its patency
Inspect and label true versus false lumen
Other factors — maximum aortic calibre, trauma, age, prior repair
Notify the referring provider directly
Management
| Scenario | Management |
|---|---|
| Type A | Emergency open surgical repair. Untreated mortality is approximately 1%–2% per hour in the early hours. |
| Type B, uncomplicated | Anti-impulse medical therapy — intravenous beta-blockade first, targeting heart rate < 60 bpm and systolic BP 100–120 mmHg — plus surveillance imaging. |
| Type B, complicated | TEVAR is preferred over open repair. “Complicated” means rupture, malperfusion, rapid aortic expansion, refractory pain, or refractory hypertension. |
| Type A IMH | Generally managed as for type A dissection, i.e. surgically, particularly with high-risk features or intractable pain. |
| Type B IMH | Medical therapy with imaging follow-up if uncomplicated; TEVAR if complicated. |
Two themes are new enough in the 2022 guideline to be worth flagging in multidisciplinary discussion: care should be delivered by a multidisciplinary aortic team, and outcomes correlate with institutional procedural volume, which supports transfer to a high-volume centre where feasible.[1]
Access the case above as a full DICOM image set, including the report impression: Aortic dissection full DICOM set.
Frequently asked questions
What is the difference between Stanford type A and type B aortic dissection?
Type A involves the ascending aorta regardless of where the entry tear is; type B does not. The distinction is made on the segment involved, not on the tear location, and it separates an emergency surgical problem from one that is usually medical in the first instance.
How do you tell the true lumen from the false lumen on CT?
The true lumen is smaller, rounder, opacifies earlier and is continuous with the undissected aorta. The false lumen is larger and crescentic, opacifies later, thromboses more often, and shows the beak and cobweb signs. The beak sign is the most dependable single feature.
Why is a non-contrast CT needed for suspected aortic dissection?
Because intramural hematoma is only reliably visible before contrast, as a crescentic hyperattenuating (≈60–70 HU) thickening of the aortic wall. After contrast it becomes inconspicuous next to the opacified lumen, and the diagnosis is missed.
What makes a type B dissection “complicated”?
Rupture, malperfusion of a branch territory, rapid aortic expansion, refractory pain, or refractory hypertension. Any of these shifts management from medical therapy to intervention, with TEVAR preferred over open repair.
Can a chest X-ray rule out aortic dissection?
No. A widened mediastinum above 8 cm raises suspicion, but a normal chest radiograph does not exclude dissection and should never delay CT angiography in a patient with a suggestive presentation.
References
- Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. Circulation. 2022;146(24):e334–e482. PMID: 36322642. doi:10.1161/CIR.0000000000001106
- Expert Panel on Cardiac Imaging; Kicska GA, Hurwitz Koweek LM, Ghoshhajra BB, et al. ACR Appropriateness Criteria® Suspected Acute Aortic Syndrome. J Am Coll Radiol. 2021;18(11S):S474–S481. PMID: 34794601. doi:10.1016/j.jacr.2021.09.004
- Murillo H, Molvin L, Chin AS, Fleischmann D. Aortic Dissection and Other Acute Aortic Syndromes: Diagnostic Imaging Findings from Acute to Chronic Longitudinal Progression. RadioGraphics. 2021;41(2):425–446. PMID: 33646901. doi:10.1148/rg.2021200138
- Sica G, Rea G, Lieto R, et al. CT diagnosis and destiny of acute aortic intramural hematoma. Front Radiol. 2025;5:1552644. PMID: 40134989. doi:10.3389/fradi.2025.1552644
- Arslan Ü, Jalalzai I. A Narrative Review of Biomarkers and Imaging in the Diagnosis of Acute Aortic Syndrome. Diagnostics (Basel). 2025;15(2):183. PMID: 39857067. doi:10.3390/diagnostics15020183

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
It’s good to see writing that is so good that you know the writer has done the homework on the subject. I am impressed with your insight and viewpoints on this topic.
Glad you liked the post, Terrance.