
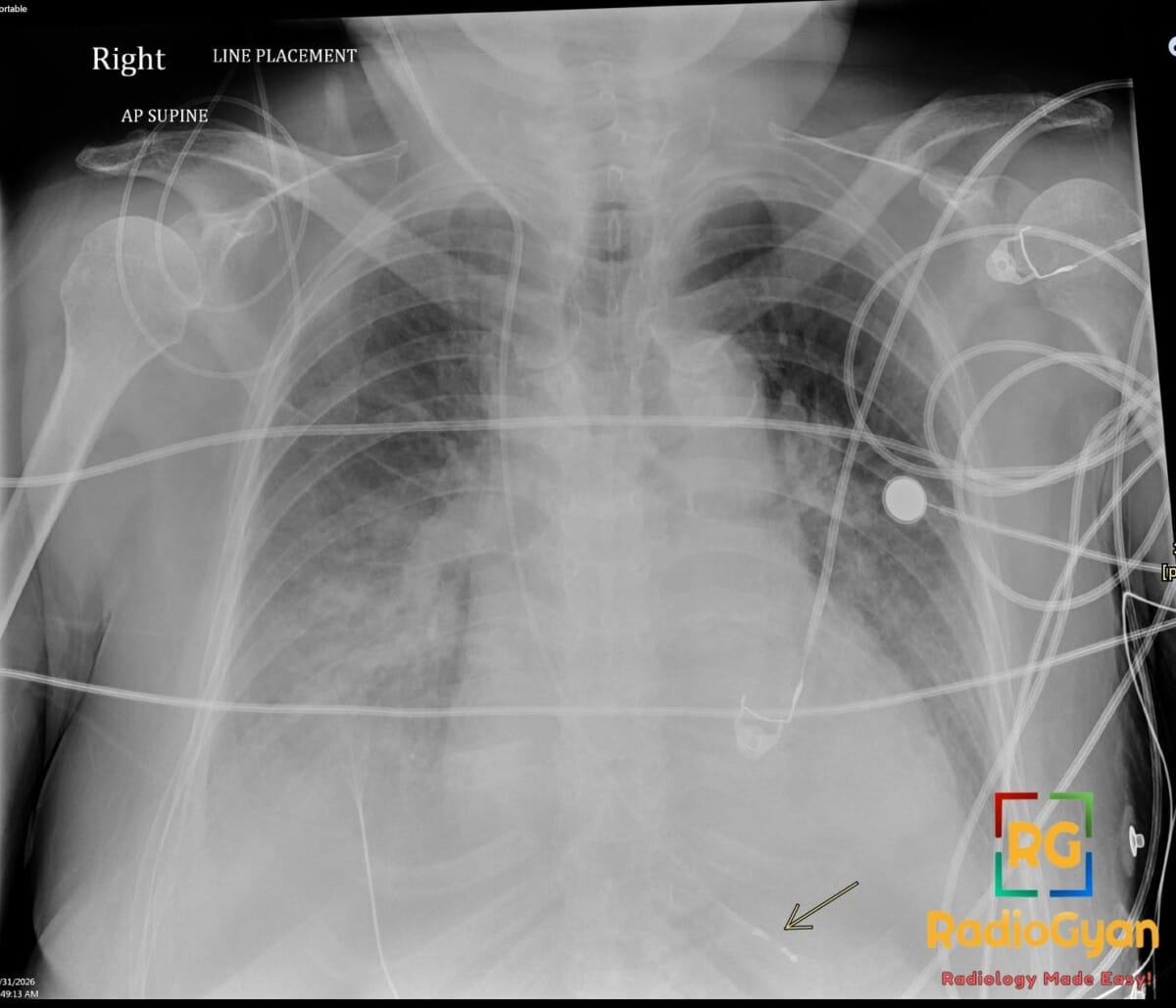
72 yr male with hemodynamically unstable bradycardia and a portable chest radiograph to evaluate device placement.
Diagnosis and teaching points:
Diagnosis: Right Internal Jugular Temporary Transvenous Pacemaker
Key facts for boards exams:
- Indicated for hemodynamically unstable bradyarrhythmias, most commonly in elderly patients with high-grade AV blocks.
- The right internal jugular vein is the preferred access site as it provides the most direct anatomical route to the right ventricle.
- On a frontal radiograph, the lead tip should be positioned at the apex of the right ventricle, appearing to the left of the spine.
- Lead perforation of the right ventricular wall occurs in approximately 1% of temporary cases but is seen in up to 6% of leads evaluated by CT.
- Twiddler’s syndrome refers to lead coiling or curling caused by patient manipulation of the device.
Detailed teaching points:
- Clinical: Typically seen in patients in their 70s-80s presenting with symptomatic bradycardia, complete heart block, or fatigability.
- Etiology/Pathophys: Lifesaving device that bypasses the native conduction system to deliver electrical stimulation directly to the right ventricular endocardium to restore cardiac output.
- Radiograph: Shows a radiopaque lead entering via the right internal jugular vein, traveling through the right atrium, and terminating at the right ventricular apex; must be monitored for kinks, fractures, or malposition.
- US: Echocardiography is used to detect complications such as pericardial effusion or cardiac tamponade resulting from lead perforation.
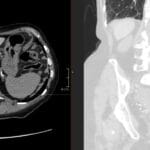
- CT: Standard modality for evaluating lead perforation; can visualize the lead tip relative to the right ventricular free wall and associated pericardial fluid.
- MRI: Devices must be specifically labeled as MRI conditional to be safe for imaging; characteristic markings on the device may indicate compatibility.
- Signs: Right Ventriculography (RVG) can identify lead perforation by showing the lead tip penetrating the right ventricular free wall.
- Frameworks: Classification of fixation includes passive (tines caught in trabeculae) or active; the right internal jugular approach is the clinical gold standard due to high success rates.
- DDx: Permanent pacemaker (subcutaneous generator, different configuration); Central venous catheter (no electrode/generator); Pulmonary artery catheter (tip in pulmonary vasculature); Lead fracture (visible discontinuity).
- Tx: Standard management includes lead repositioning if malposed, surgical intervention for severe perforation/tamponade, and eventual transition to a permanent or leadless pacemaker system.
OSCE Questions
Question: What is the preferred anatomical site for venous entry when placing this device to ensure the most direct route to the right ventricle?
Right internal jugular vein.
Question: Where should the radio-opaque tip of the lead be ideally positioned on a frontal chest radiograph?
The apex of the right ventricle.
Question: Which imaging modality is most sensitive for detecting lead perforation and evaluating the lead tip’s relationship to the ventricular wall?
Computed Tomography (CT).
Question: What is the most serious potential complication if the lead tip is seen outside the cardiac silhouette on a follow-up radiograph?
Myocardial perforation with cardiac tamponade.
Question: What are the two primary clinical indications for the emergency placement of this condition?
Hemodynamically unstable bradyarrhythmias and high-grade atrioventricular block.
MCQ Questions
1. What is the optimal radiographic position for this device tip?
A. Right atrium
B. Right ventricular apex
C. Pulmonary artery
D. Left ventricle
Answer: B. Right ventricular apex. On a frontal chest X-ray, the lead tip should ideally terminate at the right ventricular apex.
2. Which entry site offers the most direct route for this procedure?
A. Left subclavian vein
B. Right femoral vein
C. Right internal jugular vein
D. Left internal jugular vein
Answer: C. Right internal jugular vein. The right internal jugular vein provides the most direct anatomical path to the right ventricle.
3. Which imaging finding most strongly suggests lead perforation?
A. Right atrial coiling
B. New pericardial effusion
C. Superior vena cava kinking
D. Tip at cardiac apex
Answer: B. New pericardial effusion. A new or enlarging pericardial effusion on CT or ultrasound is a primary sign of ventricular perforation.
4. What is the most common clinical indication for this temporary device?
A. Asymptomatic sinus bradycardia
B. Hemodynamically unstable bradyarrhythmia
C. Decompensated heart failure
D. Acute myocardial infarction
Answer: B. Hemodynamically unstable bradyarrhythmia. Temporary transvenous pacing is primarily indicated for patients with life-threatening or hemodynamically unstable bradycardia.
5. How is this pathology primarily distinguished from a permanent pacemaker?
A. Presence of lead tines
B. Radiopaque lead material
C. Lack of subcutaneous generator
D. Right-sided venous access
Answer: C. Lack of subcutaneous generator. Temporary pacemakers utilize an external generator rather than a surgically implanted subcutaneous chest wall generator.
Check out more such cases:





Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case