
62 yr male presenting with chronic vague abdominal pain, weight loss, and a palpable right-sided abdominal fullness.
Diagnosis and teaching points:
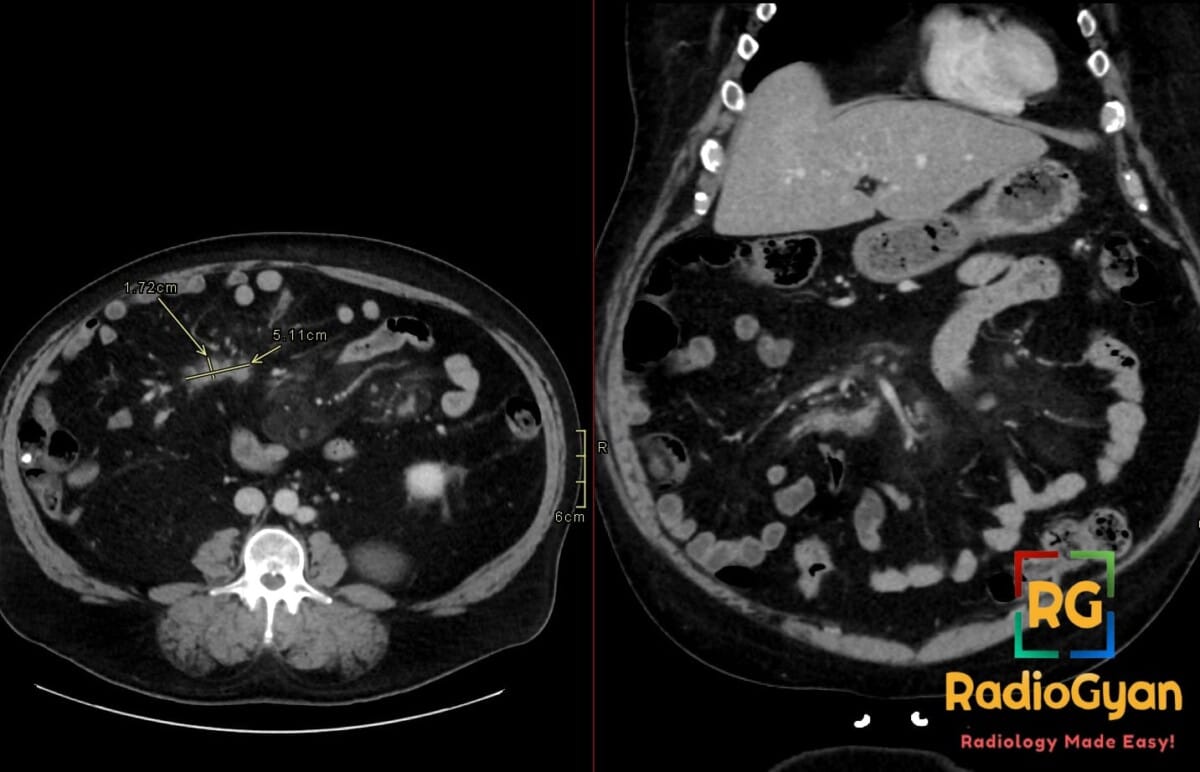
Diagnosis: Mesenteric panniculitis with developing lymphoma in the right paramidline mesentery
Key facts for boards exams:
- The fat halo sign and tumoral pseudocapsule are hallmark CT findings of mesenteric panniculitis that help differentiate it from infiltrative processes like lymphoma.
- Evolution into lymphoma should be suspected if follow-up imaging demonstrates lymph nodes larger than 12 mm, loss of the fat halo sign, or coalescence of nodes into a solid mass.
- While mesenteric panniculitis usually shows minimal or no FDG uptake, development of lymphoma typically results in high FDG-PET avidity.
Detailed teaching points:
- Clinical: Typically affects adults around age 60; 2:1 male predominance; may be asymptomatic or present with abdominal pain, weight loss, and bowel obstruction; possibly associated with malignancy in 15% of cases.
- Etiology/Pathophys: Rare idiopathic inflammatory spectrum of sclerosing mesenteritis involving chronic nonspecific inflammation of mesenteric fat with lipid-laden macrophages and variable fibrosis.
- Radiograph: Nonspecific findings including bowel displacement, calcifications, or mass effect; not a primary diagnostic modality.
- US: Often limited by bowel gas; may show hypoechoic mesenteric masses or nodular thickening but is technically challenging and unreliable.
- CT: Misty mesentery appearance with increased fat attenuation (-50 to -90 HU); well-defined mass often in the left paramidline; presence of small lymph nodes (<10 mm); development of lymphoma suggested by nodes >12 mm, nodal coalescence, and necrosis.
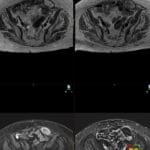
- MRI: Mesenteric mass is hypointense on T1 and variable on T2; fat-saturated T2 sequences highlight the mass as high signal; peripheral fibrotic pseudocapsule appears hypointense.
- Nuc Med: Mesenteric panniculitis shows low or no FDG avidity; PET is highly useful to identify evolving lymphoma which is typically FDG-avid.
- Signs: Fat halo sign (preserved normal fat density around vessels/nodes); Tumoral pseudocapsule (peripheral soft-tissue band of fibrosis); Misty mesentery (hazy increased fat attenuation).
- Frameworks: Characterized within the sclerosing mesenteritis spectrum: mesenteric lipodystrophy (macrophage-rich), mesenteric panniculitis (inflammation-rich), and retractile mesenteritis (fibrosis-rich).
- DDx: Lymphoma (larger nodes, no fat halo, retroperitoneal involvement); Carcinomatosis (ascites, primary tumor site); Desmoid tumor (solid fibrotic growth); Mesenteric edema (diffuse, associated with heart failure).
- Tx: Conservative observation for asymptomatic cases; symptomatic cases treated with corticosteroids, tamoxifen, or immunosuppressants; lymphoma requires systemic chemotherapy.
OSCE Questions
Question: What refers to the preservation of a normal fat rim around mesenteric vessels and lymph nodes within the inflamed mass?
Fat halo sign (or fat ring sign).
Question: When this pathology is observed on CT, what is the significance of a “tumoral pseudocapsule”?
It represents a peripheral curvilinear soft-tissue band of fibrosis that helps differentiate it from other infiltrative processes.
Question: What lymph node size threshold should raise suspicion for the development of a secondary malignancy or an alternative diagnosis like lymphoma?
Nodes greater than 10 to 12 mm in short-axis diameter.
Question: Which nuclear medicine modality is most useful for differentiating this idiopathic inflammatory condition from an evolving malignancy?
FDG-PET/CT.
Question: This condition exists on a spectrum of “sclerosing mesenteritis”; what is the term used when fibrosis and retraction of bowel loops become the predominant features?
Retractile mesenteritis.
MCQ Questions
1. Which CT sign suggests preservation of normal fat around vessels in this condition?
A. Sandwich sign
B. Fat halo sign
C. Misty mesentery
D. Tumoral pseudocapsule
Answer: B. Fat halo sign. This sign represents the preservation of normal fat density immediately surrounding mesenteric vessels and lymph nodes.
2. What lymph node size threshold suggests evolution into malignancy in this pathology?
A. Greater than 5 mm
B. Greater than 8 mm
C. Greater than 12 mm
D. Greater than 20 mm
Answer: C. Greater than 12 mm. Nodes larger than 10-12 mm or the loss of the fat halo sign raise suspicion for lymphoma.
3. Which imaging feature characterizes the “misty mesentery” appearance?
A. Diffuse anechoic fluid
B. Hazy increase in fat attenuation
C. Multiple calcified granulomas
D. Solid spiculated mass
Answer: B. Hazy increase in fat attenuation. Misty mesentery refers to a segmental increase in mesenteric fat density due to inflammation or infiltration.
4. Which modality best differentiates this inflammatory process from lymphoma?
A. Ultrasound
B. Plain film radiography
C. FDG-PET/CT
D. Non-contrast CT
Answer: C. FDG-PET/CT. Mesenteric panniculitis typically shows low FDG uptake, whereas evolving lymphoma is usually FDG-avid.
5. What does a peripheral soft-tissue band encasing the mesenteric mass represent?
A. Acute hemorrhage
B. Tumoral pseudocapsule
C. Vascular encasement
D. Bowel wall thickening
Answer: B. Tumoral pseudocapsule. This curvilinear band represents a peripheral layer of fibrosis that limits the inflamed mesenteric fat.
Check out more such cases:



Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case