
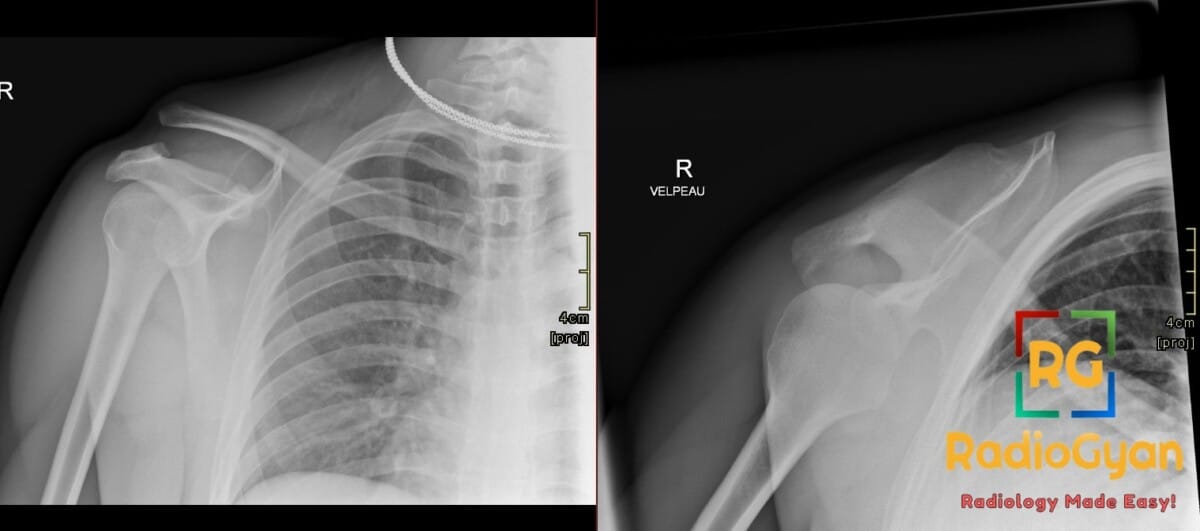
25 yr male presenting with localized shoulder pain and superior clavicular deformity following a fall during a rugby match.
Diagnosis and teaching points:
Diagnosis: Right acromioclavicular joint injury
Key facts for boards exams:
- The Rockwood classification (Types I-VI) is the gold standard for staging, distinguishing injuries based on acromioclavicular and coracoclavicular ligament integrity and the direction/degree of clavicular displacement.
- A normal coracoclavicular (CC) distance is 11-13 mm; a distance ≥12 mm or a >25% increase compared to the contralateral side is considered pathologic for higher-grade injuries.
- The Zanca view, performed with a 10-15° cephalad tilt and 50% reduced penetration, is the optimal radiographic projection to visualize the acromioclavicular joint without overlying structures.
Detailed teaching points:
- Clinical: Most common in active males aged 20-40 years involved in contact sports; presents with localized AC joint pain, swelling, and a visible step-off deformity in higher-grade injuries.
- Etiology/Pathophys: Results from a direct fall onto the superior acromion or an indirect force via arm traction, causing disruption of the AC ligaments (primary stabilizers) and CC ligaments (vertical stabilizers).
- Radiograph: Findings include AC joint widening (>7 mm), increased CC distance, and superior displacement of the distal clavicle; weight-bearing stress views can help differentiate stable Type II from unstable Type III injuries.
- MRI: Essential for Evaluating ligamentous integrity and muscle detachment (deltoid/trapezius); often used to reclassify radiographic findings by detecting soft tissue details like bone marrow edema and joint effusion.
- Signs: Step deformity refers to the vertical misalignment between the inferior borders of the acromion and distal clavicle on an AP view; Zanca sign utilizes a specific radiographic angle to highlight joint space widening.
- Frameworks: Rockwood Classification: Type I (sprain), Type II (AC rupture, CC sprain), Type III (AC/CC rupture, 25-100% displacement), Type IV (posterior displacement), Type V (>100% superior displacement), Type VI (inferior displacement).
- DDx: AC joint osteoarthritis (shows narrowing/osteophytes rather than widening), distal clavicle fracture (demonstrates cortical disruption), and rotator cuff tears (tendon pathology rather than joint displacement).
- Tx: Types I and II are managed conservatively with slings and physical therapy; Types IV, V, and VI typically require surgical reconstruction; Type III management is controversial and tailored to the patient’s activity level.
OSCE Questions
Question: Which classification system is used to grade the severity of this pathology based on ligamentous disruption and clavicle displacement?
The Rockwood classification.
Question: What specific radiographic view involving a 10-15 degree cephalad tilt is used to optimize visualization of this joint?
The Zanca view.
Question: An increase in the coracoclavicular (CC) distance to what percentage of the contralateral side distinguishes a Type V injury from a Type III injury?
Greater than 100 percent increase.
Question: Which radiographic view is essential to diagnose a Type IV injury, characterized by posterior displacement of the clavicle?
Axillary lateral view.
Question: What is the threshold measurement for the coracoclavicular (CC) distance beyond which the joint is considered pathologic?
A distance of 12 mm or greater.
MCQ Questions
1. What is the normal maximum coracoclavicular distance?
A. 5 mm
B. 9 mm
C. 13 mm
D. 18 mm
Answer: C. 13 mm. Normal coracoclavicular distance is typically between 11 mm and 13 mm.
2. Which radiographic view best detects posterior displacement?
A. Zanca view
B. Axillary view
C. Grashey view
D. AP weight-bearing view
Answer: B. Axillary view. The axillary view is required to identify Type IV injuries involving posterior clavicular displacement.
3. Which finding defines a Rockwood Type V injury?
A. AC ligament sprain only
B. Posterior clavicle displacement
C. 25-100% CC distance increase
D. >100% CC distance increase
Answer: D. >100% CC distance increase. Type V injuries are characterized by severe vertical displacement exceeding 100% of the normal CC interval.
4. What characterizes a Rockwood Type II injury?
A. Ruptured CC ligaments
B. Normal AC joint interval
C. Intact AC, ruptured CC
D. Ruptured AC, sprained CC
Answer: D. Ruptured AC, sprained CC. In Type II, the AC ligaments are torn while the CC ligaments remain functionally intact but sprained.
5. How is the Zanca view performed?
A. 45° caudal tilt
B. 10-15° cephalad tilt
C. 30° internal rotation
D. 90° abduction
Answer: B. 10-15° cephalad tilt. The Zanca view uses a 10-15° cephalad tilt and reduced voltage to better visualize the joint.
Check out more such cases:





Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case