
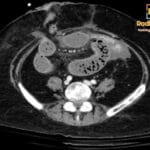
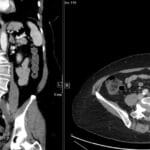
62 yr female presenting with a palpable right lower quadrant mass and chronic abdominal pain.

Diagnosis and teaching points:
Diagnosis: Appendiceal Mucocele
Key facts for boards exams:
- Characterized by an appendiceal outer-to-outer diameter of 15 mm or greater, which is the diagnostic threshold to distinguish it from acute appendicitis.
- The “Onion-skin sign” on ultrasound is considered pathognomonic, representing multiple echogenic layers of inspissated mucin.
- Wall calcification on CT is highly specific for the diagnosis, though present in less than 50% of cases.
- Clinical: Middle-aged to elderly populations; 50% are asymptomatic; symptomatic cases present with a palpable right lower quadrant mass, abdominal pain, or pelvic pain.
- Etiology/Pathophys: Chronic transformation of the appendix into a mucus-filled sac due to luminal obstruction; causes include retention cysts, appendicoliths, adhesions, fibrosis, or neoplasms.
- US: Elongated tubular mass in the right lower quadrant; characteristic “onion-skin” texture with internal echogenic layers; “drumstick” or “pear-shaped” appearance; no internal blood flow on Doppler; mucinous ascites from rupture appears as low-level echoes with ill-defined septations.
- CT: Round or tubular low-attenuation (17-26 HU) cystic mass near water density; well-encapsulated; wall calcification is a strong diagnostic feature; wall irregularity and mural nodularity suggest malignancy (cystadenocarcinoma).
- MRI: Tubular cystic structure; T2-weighted images show high signal intensity depending on protein/mucin content; helps differentiate from ovarian or tubal pathology by demonstrating the relationship to surrounding anatomy.
- Signs: Onion-Skin Sign: Pathognomonic ultrasound finding of multiple echogenic layers; Whorly/Onion Peel Appearance: CT description of layered mucin within the dilated lumen.
- Frameworks: Diagnostic criteria: Appendicular diameter ≥15 mm (83% sensitivity, 92% specificity for mucocele versus 6 mm for appendicitis).
- DDx: Hydrosalpinx (lacks onion-skin sign); Tubo-ovarian abscess (fever, complex appearance); Acute appendicitis (diameter <15 mm, inflammatory clinical picture); Ovarian pathology (distinct anatomical origin on MRI).
- Tx: Appendectomy is the primary treatment to prevent rupture; debulking surgery and intraperitoneal chemotherapy are required if pseudomyxoma peritonei (rupture) occurs.
OSCE Questions
Question: What is the pathognomonic ultrasound sign described as multiple echogenic layers within the mass?
The “onion-skin” sign.
Question: What is the minimum appendicular diameter threshold used to suggest this diagnosis over acute appendicitis?
15 mm.
Question: Which CT finding, although present in less than 50% of cases, strongly supports the diagnosis of this condition?
Wall calcification.
Question: What serious complication, characterized by diffuse gelatinous ascites, can occur if this lesion ruptures?
Pseudomyxoma peritonei.
Question: On CT or MRI, which specific morphological features are statistically significant indicators of malignancy in this pathology?
Wall irregularity and soft-tissue thickening or mural nodularity.
MCQ Questions
1. Which ultrasound finding is considered pathognomonic for this pathology?
A. Acoustic shadowing
B. Comet-tail artifact
C. Onion-skin sign
D. Target sign
Answer: C. Onion-skin sign. The layered echogenic appearance caused by inspissated mucin is a diagnostic hallmark of appendiceal mucocele.
2. What is the minimum diameter threshold for diagnosing this condition over acute appendicitis?
A. 6 mm
B. 10 mm
C. 15 mm
D. 20 mm
Answer: C. 15 mm. An outer diameter of 15 mm or greater is the specific threshold for diagnosing a mucocele.
3. Which CT feature most strongly supports the diagnosis of this pathology?
A. Perappendiceal fat stranding
B. Peripheral wall calcification
C. Enhancing internal septations
D. Air-fluid levels
Answer: B. Peripheral wall calcification. Curvilinear wall calcification is a highly suggestive feature of an appendiceal mucocele on CT imaging.
4. Rupture of this specific mass may lead to which serious clinical complication?
A. Portal vein thrombosis
B. Pseudomyxoma peritonei
C. Hepatic encephalopathy
D. Meckel’s diverticulitis
Answer: B. Pseudomyxoma peritonei. Rupture of a mucinous appendiceal tumor can result in the intraperitoneal spread of gelatinous ascites.
5. Why is ultrasound-guided fine needle aspiration contraindicated for this lesion?
A. Risk of hemorrhage
B. Risk of mucinous dissemination
C. High false-negative rate
D. Risk of bowel perforation
Answer: B. Risk of mucinous dissemination. Aspiration is avoided to prevent the iatrogenic seeding of mucus and potentially malignant cells into the peritoneum.
Check out more such cases:




Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case