TIRADS-Klassifizierungstabelle
|
| Kategorie |
Punkte |
Verdacht |
Malignitätsrisiko |
Richtlinie |
| TR1 |
0 |
Gutartig |
0.3% |
Keine FNA |
| TR2 |
2 |
Nicht verdächtig |
1.5% |
Keine FNA |
| TR3 |
3 |
Leicht verdächtig |
4.8% |
Wenn ≥2,5 cm: FNA Wenn ≥1,5 cm: Nachuntersuchung nach 1, 3, 5 Jahren
|
| TR4 |
4-6 |
Mäßig verdächtig |
9.1% |
Wenn ≥1,5 cm: FNA Wenn ≥1 cm: Nachuntersuchung nach 1, 3, 5 Jahren
|
| TR5 |
7 oder mehr |
Höchst verdächtig |
35% |
Wenn ≥1 cm: FNA Bei ≥0,5 cm jährliche Nachuntersuchung über 5 Jahre
|
FNA – Feinnadelaspiration.
Risiko einer Schilddrüsenmalignität abhängig vom TIRADS-Score
- Bei Schilddrüsenknoten des Typs TR 1 liegt das Risiko einer bösartigen Erkrankung bei 0,3 %.
- TR 2 Schilddrüsenknoten haben ein Malignitätsrisiko von 1,5 %.
- Bei Schilddrüsenknoten des Typs TR 3 liegt das Risiko einer bösartigen Erkrankung bei 4,8 %.
- Bei Schilddrüsenknoten des Typs TR 4 liegt das Risiko einer bösartigen Erkrankung bei 9,1 %.
- Bei Schilddrüsenknoten des Typs TR 5 liegt das Risiko einer bösartigen Erkrankung bei 35 %.
Vorbehalte zum Schilddrüsen-Ultraschall-Rechner
- Wenn Randverkalkungen den Knoten vollständig verdecken, wählen Sie die Zusammensetzung „fest“ und die Echogenität „isoechoisch“.
- Wenn der Rand nicht bestimmt werden kann, wählen Sie „unklar definierter Rand“.
- Wenn die Echogenität nicht bestimmt werden kann, wählen Sie „isoechoisch“.
- Wenn die Zusammensetzung nicht bestimmt werden kann, wählen Sie „fest“.
- Punktförmige echogene Herde und Merkmale, die höher als breit sind, weisen die höchsten Punkte auf, bewerten Sie diese daher sorgfältig.
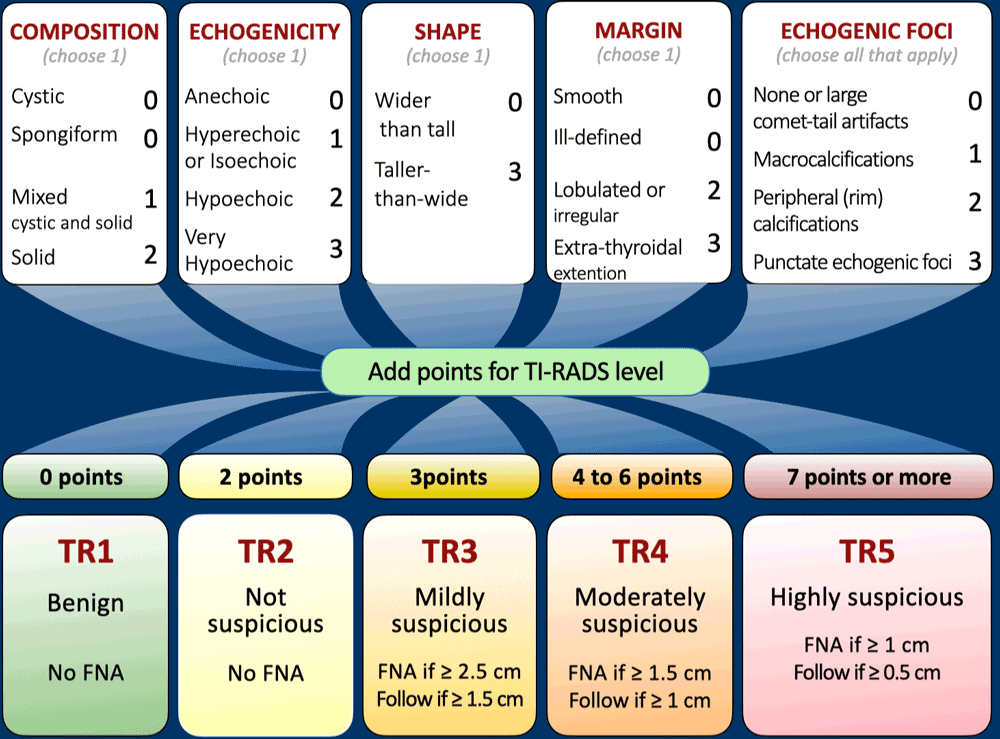
Kernpunkte aus dem ursprünglichen TIRADS-Artikel:
Zusammensetzung
Zystische oder fast vollständig zystische Knoten sind im Allgemeinen gutartig, ebenso wie spongiforme Knoten, die überwiegend aus kleinen zystischen Räumen bestehen. Feste Komponenten mit verdächtigen Merkmalen können eine weitere Abklärung auf Malignität erforderlich machen.
Echogenität
Bei der Beurteilung der Echogenität wird die Reflektivität eines Knotens mit dem benachbarten Schilddrüsengewebe verglichen. Ausnahmen sind sehr echoarme Knoten, bei denen die Riemenmuskulatur als Referenzpunkt dient. Besondere Aufmerksamkeit gilt echofreien Knoten.
Form
Eine Form, die höher als breit ist, kann bei der Beurteilung in der axialen Ebene durch Vergleich der Höhen- und Breitenmessungen sehr spezifisch für eine bösartige Erkrankung sein.
Marge
Unscharfe oder unregelmäßige Ränder, insbesondere mit Vorwölbungen oder Läppchen, sollten Verdacht erregen. Auch eine Ausdehnung über die Schilddrüsengrenze hinaus sollte in Betracht gezogen werden.
Echogene Herde
Verschiedene Arten echogener Herde sind unterschiedlich verdächtig. Punktförmige echogene Herde innerhalb fester Komponenten sind besonders besorgniserregend und sollten in Verbindung mit anderen Merkmalen untersucht werden.
Papilläre Schilddrüsenmikrokarzinome
Eine Biopsie von Knoten kleiner als 1 cm wird im Allgemeinen nicht empfohlen; Ausnahmen können jedoch unter bestimmten Umständen gemacht werden. Leitlinien raten von einer routinemäßigen Biopsie solcher kleinen Knoten ab, es sei denn, es handelt sich um eine aktive Überwachung, Ablation oder die Erwägung einer Lobektomie bei papillären Mikrokarzinomen.
Messung und Dokumentation
Eine genaue Größenbestimmung und detaillierte Dokumentation der Knotenposition sind für die Überwachung und den Vergleich im Laufe der Zeit von entscheidender Bedeutung.
Definition von Wachstum
Eine signifikante Vergrößerung wird definiert als eine 20%ige Zunahme in mindestens zwei Knotendimensionen mit einer minimalen Zunahme von 2 mm oder einer Volumenzunahme von 50% oder mehr.
Zeitpunkt der Folgesonographie
- In der Literatur herrscht kein Konsens über den optimalen Abstand für Folgesonographien bei Knoten, die die FNA-Größenkriterien nicht erfüllen.
- Scan-Intervalle von weniger als einem Jahr werden im Allgemeinen nicht empfohlen, außer bei nachgewiesenen Krebserkrankungen unter aktiver Überwachung.
- Die Nachuntersuchungsintervalle sollten auf dem ACR TI-RADS-Wert des Knotens basieren, wobei bei verdächtigeren Läsionen zusätzliche Sonogramme erforderlich sind.
- Bei TR5-Läsionen werden jährliche Scans über einen Zeitraum von bis zu 5 Jahren empfohlen.
- Bei TR4-Läsionen werden Scans nach 1, 2, 3 und 5 Jahren empfohlen.
- Bei TR3-Läsionen können nach 1, 3 und 5 Jahren Nachuntersuchungen mit Bildgebung durchgeführt werden.
- Die Bildgebung kann nach 5 Jahren abgebrochen werden, wenn keine Größenänderung eintritt, was auf ein gutartiges Verhalten hindeutet.
- Für die Behandlung von Knoten, die sich deutlich vergrößern, aber nach 5 Jahren unterhalb der FNA-Größengrenze bleiben, gibt es keine veröffentlichten Leitlinien, aber wahrscheinlich ist eine kontinuierliche Nachsorge erforderlich.
- Wenn der ACR TI-RADS-Wert eines Knotens bei der Nachuntersuchung ansteigt, sollte das nächste Sonogramm unabhängig vom Ausgangswert in einem Jahr geplant werden.
Anzahl der zu biopsierenden Knoten
Um unnötige Eingriffe und Beschwerden für den Patienten zu vermeiden, wird eine Biopsie der beiden Knoten mit dem verdächtigsten Erscheinungsbild empfohlen.
Beurteilung der zervikalen Lymphknoten
Spezifische Merkmale, die auf Metastasen hinweisen, sollten eine FNA verdächtiger Knoten sowie von bis zu zwei Knoten veranlassen, die die Biopsiekriterien gemäß den ACR TI-RADS-Richtlinien erfüllen.
TI-RADS FAQ
Wofür steht TI-RADS?
TI-RADS steht für Thyroid Imaging Reporting and Data System (Schilddrüsenbildgebungs-, Berichts- und Datensystem). Es standardisiert die Ultraschallbefundung und das Management von Schilddrüsenknoten mithilfe eines punktbasierten Systems des American College of Radiology (ACR).
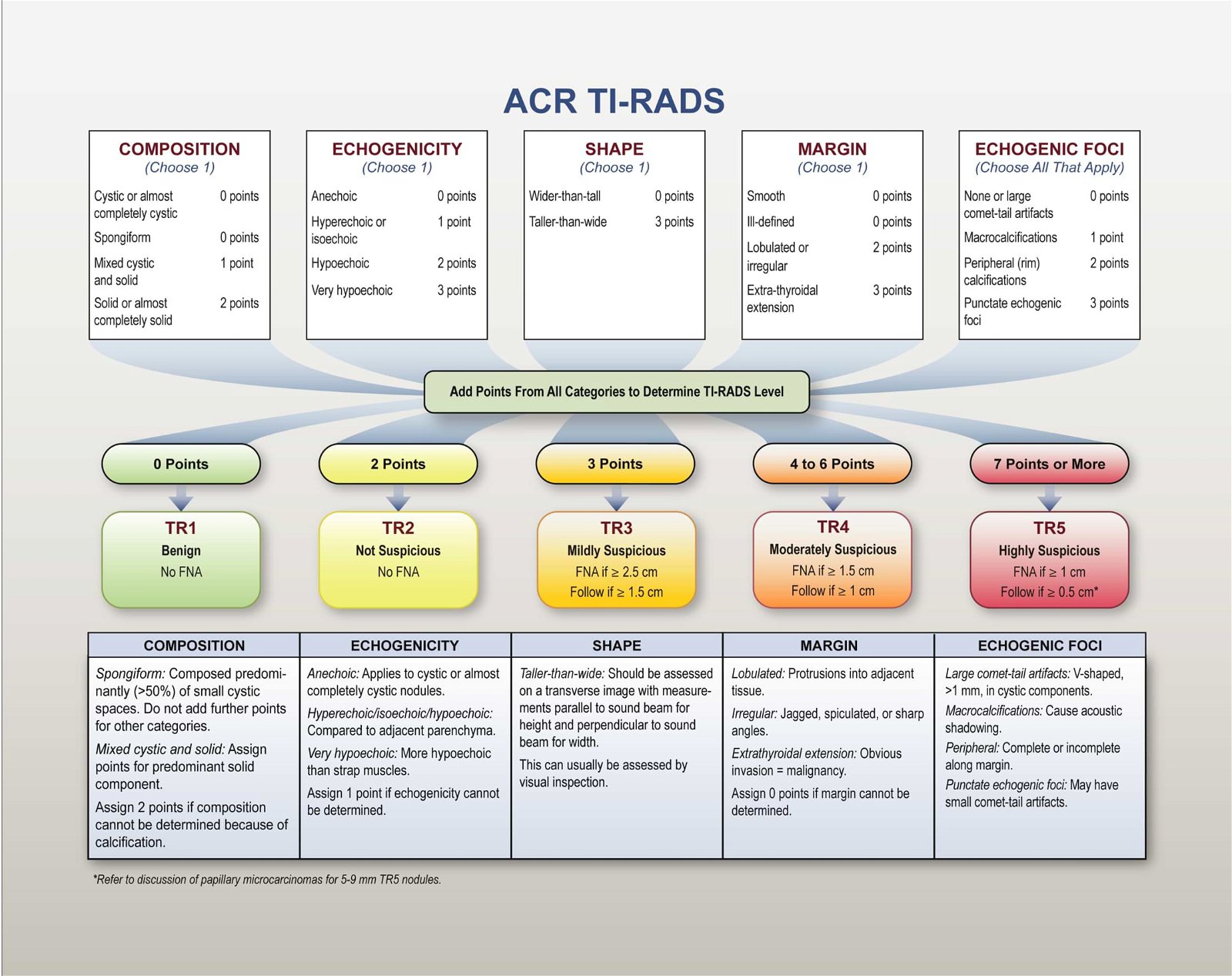
Wie benutze ich den TI-RADS-Taschenrechner?
1) Führen Sie eine vollständige Schilddrüsen-Sonographie durch. 2) Wählen Sie Merkmale hinsichtlich Zusammensetzung, Echogenität, Form, Begrenzung und echogener Herde aus. 3) Überprüfen Sie die Gesamtpunktzahl und die TI-RADS-Kategorie. 4) Befolgen Sie die größenbasierten Empfehlungen für die Nachsorge oder Feinnadelaspiration.
Was sind die TI-RADS-Kategorien?
TR1 Gutartig, TR2 Nicht verdächtig, TR3 Leicht verdächtig, TR4 Mäßig verdächtig, TR5 Hoch verdächtig. Die Kategorie wird anhand der Gesamtpunktzahl der sonografischen Merkmale bestimmt.
Welche Ultraschallmerkmale werden beurteilt?
Fünf Bereiche: Zusammensetzung, Echogenität, Form (transversal), Rand und echogene Herde. Jeder Bereich trägt Punkte bei, die sich zu einer TI-RADS-Kategorie summieren.
Wann sollte eine Feinnadelaspiration durchgeführt werden?
Typische ACR-Größenschwellenwerte: TR3 erwägt FNA ≥ 2,5 cm; TR4 erwägt FNA ≥ 1,5 cm; TR5 empfiehlt FNA ≥ 1,0 cm. Klinisches Urteilsvermögen ist stets anzuwenden.
Was sind Nachbeobachtungsintervalle?
Übliches Vorgehen: TR1–TR2: keine routinemäßige Nachsorge; TR3: Ultraschalluntersuchung nach ca. 12 Monaten; TR4: Ultraschalluntersuchung nach 6–12 Monaten; TR5: Ultraschalluntersuchung nach 3–6 Monaten, falls keine Biopsie durchgeführt wurde. Anpassung je nach Größe und Risiko.
Wie genau ist TI-RADS?
ACR TI-RADS ist validiert und weit verbreitet; es verbessert die Konsistenz und reduziert unnötige Biopsien. Die Genauigkeit hängt von der Bildqualität und der korrekten Merkmalsauswahl ab; sie ersetzt jedoch nicht die klinische Beurteilung.
Welche Merkmale deuten auf Gutartigkeit hin?
Spongiforme Zusammensetzung, anechogene/zystische Knötchen, hyperechogene/isoechogene Echogenität, breiter als hoch, glatte Ränder und große Kometenschweif-Artefakte in den zystischen Komponenten.
Welche Merkmale erwecken Verdacht?
Sehr hypoechogene Echogenität, solide Zusammensetzung, höher als breit, unregelmäßige/gelappte Ränder, punktförmige echogene Herde, periphere/makrokalzifizierte Strukturen und extrathyreoidale Ausdehnung.
Welche Einschränkungen hat TI-RADS?
Ultraschallbasiertes System; Variabilität zwischen verschiedenen Untersuchern; berücksichtigt keine klinischen Risikofaktoren oder die Wachstumsrate; weniger zuverlässig bei diffuser Erkrankung. Anwendung nur im klinischen Kontext.
Basieren diese Tools auf den ACR-Richtlinien?
Ja, die Bewertung entspricht den ACR TI-RADS-Whitepapers und dem zugehörigen Glossar. Das Tool dient Schulungszwecken und wird nicht offiziell von der ACR empfohlen.
Wie wendet man TI-RADS bei multinodulärer Schilddrüse an?
Bewerten Sie jeden Knoten einzeln. Führen Sie jeweils eine Feinnadelaspiration bei maximal zwei Knoten mit den höchsten Punktwerten durch; verfolgen Sie maximal vier Knoten mit den höchsten Punktwerten.
Hat die Knotengröße Einfluss auf die Behandlung?
Die Größe hat keinen Einfluss auf den TI-RADS-Score, bestimmt aber die Behandlungsschwellen für die Feinnadelaspiration und die Nachsorge. Größere Knoten in höheren Kategorien erfordern ein früheres Eingreifen.
Wer hat diesen Taschenrechner entwickelt?
Dieser TI-RADS-Rechner wurde von Dr. Amar Udare, MD, DNB, einem Facharzt für Radiologie und klinischen außerordentlichen Professor für diagnostische Bildgebung (Radiologie) an der Universität von Calgary, entwickelt und wird von ihm betreut.
Erklärung des Schilddrüsen-Ultraschall-Scores
Eine ausführlichere Anleitung mit Beispielen finden Sie in diesem Artikel:
TIRADS ACR: Was Radiologen wissen müssen!
Mehr Ressourcen



Über den Autor
Dr. Amar Udare, MD, DNB
Dr. Udare besitzt einen MBBS- und MD-Abschluss und ist Experte im Bereich der Radiologie. Er ist Autor mehrerer von Experten begutachteter Publikationen und leistet damit einen bedeutenden Beitrag zur medizinischen Forschung. Seine Arbeiten sind auf PubMed und Google Scholar verfügbar.
Neben seinen akademischen und beruflichen Erfolgen ist Dr. Udare ein begeisterter Leser und beschäftigt sich gerne mit den neuesten Fortschritten in der Medizintechnik. Sein Engagement, komplexes medizinisches Wissen Patienten und der breiten Öffentlichkeit zugänglich zu machen, steht im Einklang mit unserer Mission bei RadioGyan.com.
Bei weiteren Fragen oder Unklarheiten können Sie sich gerne über das Kontaktformular an Dr. Udare wenden.