
Recommendation
Caveats for using the Fleishner guidelines calculator for incidental pulmonary nodules:
- Applicable for patients ≥35 years old with incidental pulmonary nodules on CT imaging.
- Not to be used for
- Lung cancer screening
- For patients with known primary cancer
- Immunocompromised patients.
- Management depends on the most suspicious lung nodule.
- IN ADULTS, all CT scans of the thorax should be reconstructed and archived with contiguous thin sections (≤1.5 mm, typically 1.0 mm) to accurately characterize and measure small pulmonary nodules. Multiplanar reformats in the sagittal and coronal planes are also recommended.
- Follow-up CT studies should be performed with a low dose protocol.
- For smaller nodules, dimensions are average of long and short axes, rounded to the nearest millimeter. Thus the size threshold (<6 mm) corresponds to a rounded measurement of 5 mm or less as per these guidelines.
- For nodules more than 10mm both long and short axes dimensions are documented.
- Volume thresholds of 100 and 250 mm3 are used for volumetry instead of the 6- and 8-mm thresholds used for linear measurements.
- Prior imaging studies should always be viewed to assess stability. Comparison between the earliest available study and the most recent study should be performed.
- All attenuation measurements for nodules should be made on the thinnest available soft-tissue window images.
- Risk Factors for Malignancy
- Nodule Size and Morphology: Larger nodules and spiculated margins are worrisome.
- Nodule Location:
- Lung cancer - Upper lobes.
- Adenocarcinoma and Mets- Peripheral portions
- Squamous cancers - Near hila
- Perifissural solid nodules are usually benign intrapulmonary lymph nodes.
- Nodule Multiplicity: Multiplicity is associated with a lower risk of malignancy especially > 5.
- Nodule Growth Rate: Volume doubling time for cancers are in the range of 100–400-day range and correspond to an increase in diameter by 26%.
- Emphysema and Fibrosis: Increased risk.
- Age, Sex, Race, and Family History
- Tobacco and Other Inhaled Carcinogens
- Follow-up CT is NOT recommended when small nodules have a perifissural or other juxtapleural location and a morphology consistent with an intrapulmonary lymph node, even if the average dimension exceeds 6 mm.
- Recommendations for nodules detected on incomplete CT chest studies, for eg. Nodules at lung bases covered on CT abdomen:
- Most small nodules (<6 mm) - No further investigation
- Intermediate-size nodules (6–8-mm) nodules- Follow-up CT of the complete chest after an appropriate interval (3–12 months depending on clinical risk) to confirm stability and to evaluate additional findings.
- Large or very suspicious nodule - Complete dedicated CT thorax examination for further evaluation.
Video Tutorial

Fleischner Society 2017 Guidelines for Management of Incidentally Detected Pulmonary Nodules in Adults
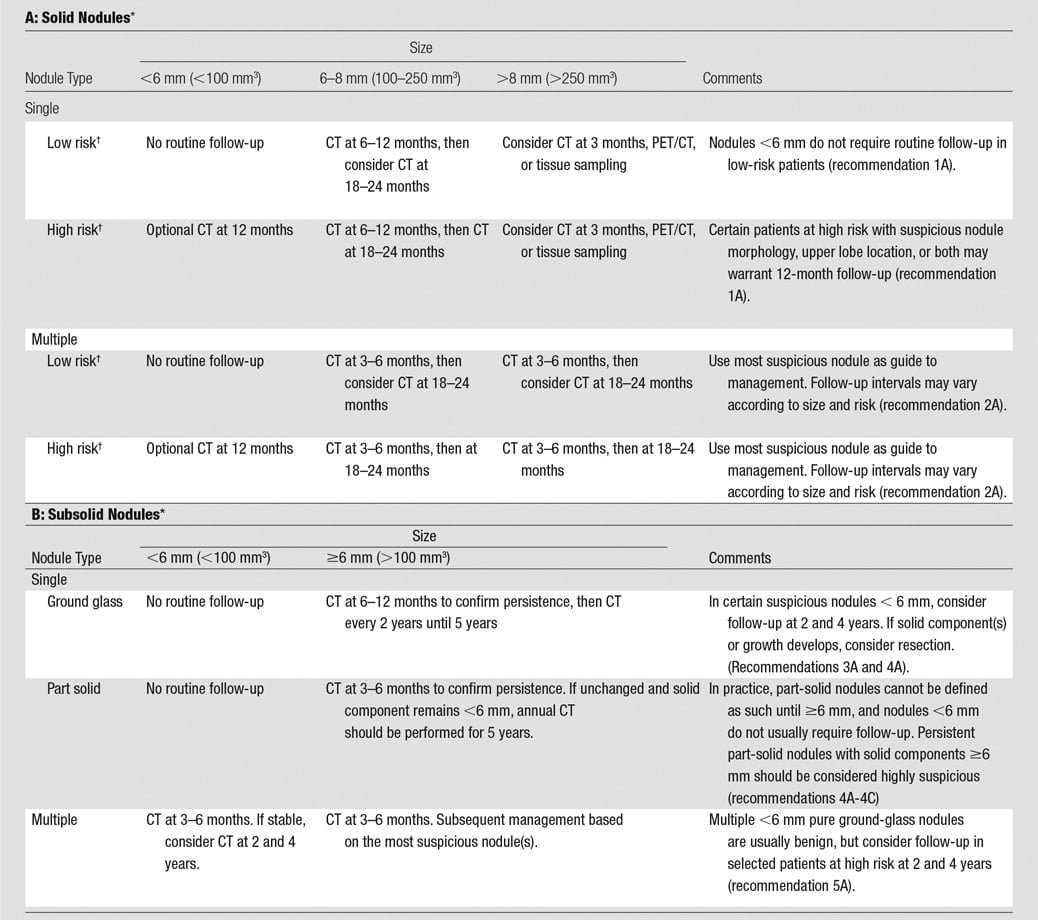
Reference: Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017 Heber MacMahon et.al. Radiology 2017 284:1, 228-243. Read the complete article here: https://pubs.rsna.org/doi/10.1148/radiol.2017161659

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
This page was last updated on

Did the recommendations change recently? I noticed for example “solid, multiple nodules, high risk” is now recommending 3-6 months with a 2year f/u if stable. When I looked at MD calc to date, Fleishner’s says options 12 months which was what it used to be on this site as well. Please advise and thank you for your time.
Thank you for your feedback.
I checked this. The guidelines have not changed as per my knowledge. For high risk solid multiple nodules less than 6mm the recommendation is do an option CT in 12 months. For nodules larger than 6mm, the recommendations are the ones you mentioned. This is as per the chart in the Fleishner article. Can you please check again and let me know?
Thank you for your reply, I appreciate it very much! I went back, you are correct. It’s odd because I looked at it a few times along with another colleague ( perhaps user error). Either way, I’m see the correct guidelines. Thanks again!
Thank you for your feedback and being thorough. Please check the other calculators and if you have any suggestions for improvement, please let me know.
With 2 subsolid lung nodule and both 6-7 mm big, when is the next follow up CT?.. My first CT was done in Feb then a follow up in May showed no change in size. does it mean my next CT is in 2 years?
Kindly discuss this with your radiologist/family doctor.