

Quiz
Normal density of mesenteric fat is
- -100 to -160 HU
- -40 to -60 HU
- 0 HU
- 100 HU
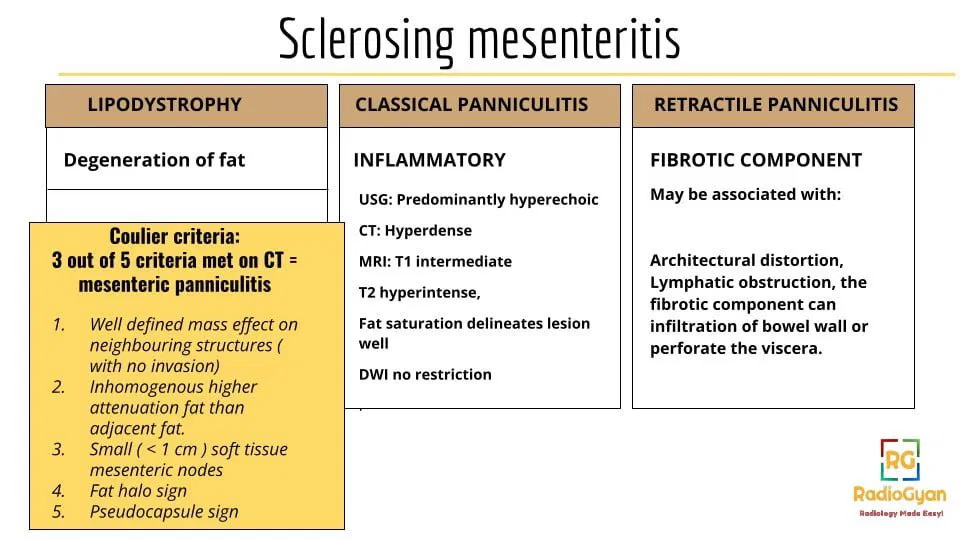
This disorder belongs to a broader group of disorders called sclerosing mesenteritis.
Pathophysiology
The aetiology is known to be largely unknown, with possibilities that have been suggested being: previous abdominal trauma, infection, autoimmunity, vasculitis and paraneoplastic syndrome.
Key Imaging Features
- Mesenteric fat changes: 90 % times involves small bowel mesentery, more commonly seen to the left of the midline (jejunal mesentery)
CT:
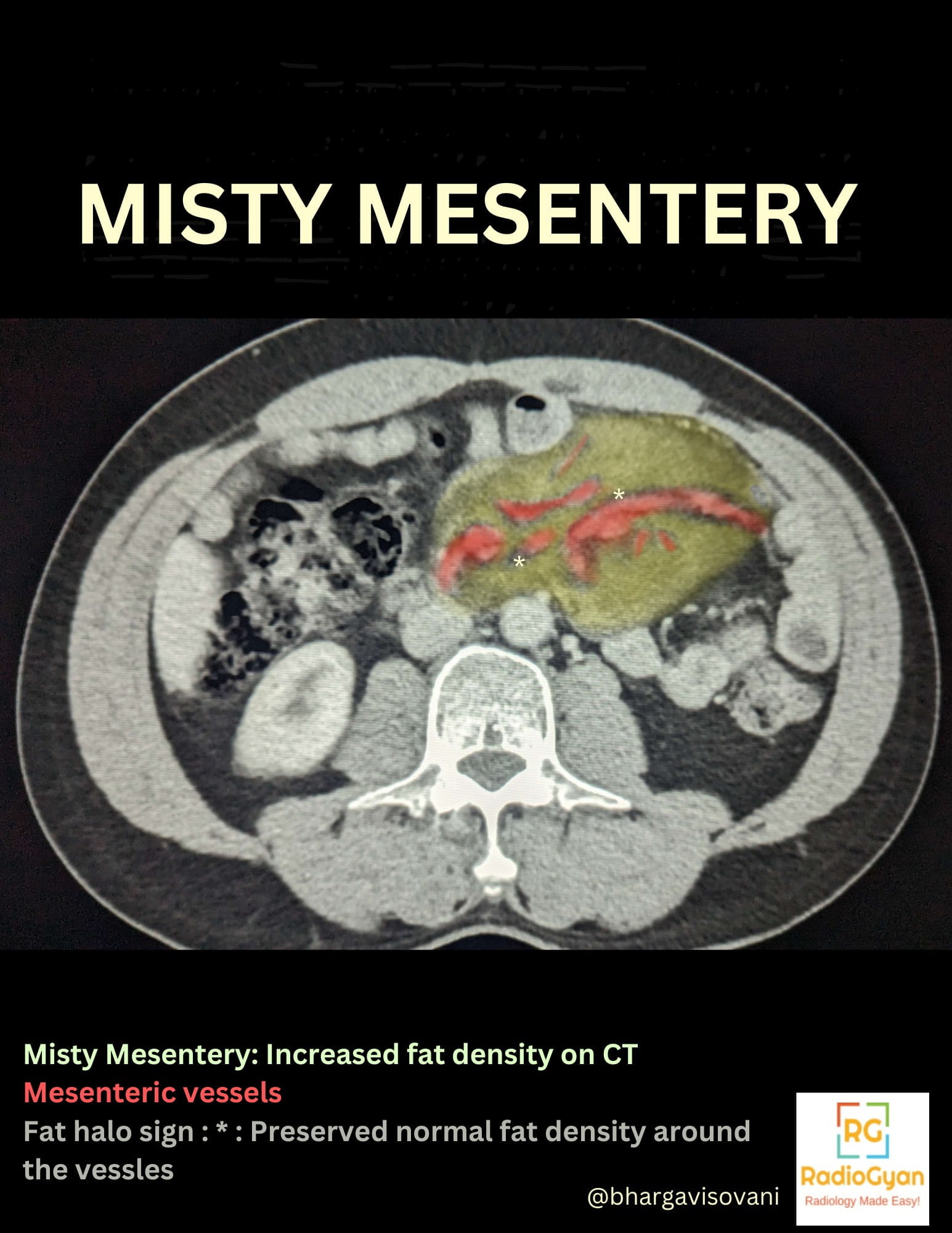
- Normal density of mesenteric fat is -100 to -160 HU.Presence of cells/edema/lymph/blood in the mesentery increases density to a minimum of -40 to -60 HU.
- Heterogeneously increased fat density on CT.
- Resultant displacement of adjacent bowel loops. (no displacement of vessels)
Specific signs:
- Tumour pseudocapsule sign : Peripheral fibrotic rim of soft-tissue attenuation around the mesenteric mass, mostly always less than 3 mm. (Also seen in mesenteric lipomatous lesions)
- Fat halo sign : Normal fat density is preserved around the mesenteric vessels.(Also seen in mesenteric lymphoma)
Ultrasound:
Corresponding region on ultrasound appears as a well defined hyperechoic area with few hypoechoic elements, or if heterogeneous echogenicity, predominantly a hyperechoic appearance.
MRI:
- In the inflammatory type, the mass appears intermediate intensity on T1 weighted images, and higher intensity on T2 weighted images.
- In the fibrotic variant of the disease, T1and T2 hypointense mass is seen, which shows delayed enhancement on post contrast images. Fat saturated images help delineate the mass better. There is no restricted diffusion on DWI.
FDG PET CT:
No uptake in mesenteric panniculitis ( neoplastic lesions are FDG avid)
B) Mesenteric lymph nodes: Enlarged nodes are seen within the regions of fat stranding.
Imaging Recommendation:
CT
Top 3 Differential Diagnosis :
- Mesenteric oedema- Findings of the aetiology like hepatic cirrhosis, renal failure, bowel ischemia
- Mesenteric haemorrhage – Hyperdense on CT ( 40 – 60 HU) and hyperintense on T1.
- Peritoneal tuberculosis – Mesenteric nodularity, peritoneal thickening, ascites and enlarged lymph nodes, and involvement of other abdominal organs.
- Non hodgkins and hodgkins tumour
- Carcinoid tumour appears similar to retractile panniculitis : (Both are soft tissue masses with calcification; however fat is preserved around the vessels in panniculitis.)
- Peritoneal carcinomatosis and peritoneal mesothelioma appear similar to retractile panniculitis, but show much more extensive peritoneal involvement, thickening and ascites.
Clinical Features :
Symptoms:
- Mostly presents as an incidental finding, with patients being asymptomatic.
- Less commonly may present as abdominal pain, nausea, vomiting, diarrhoea, bloating, weight loss.
- Few may reveal a palpable abdominal mass.
Age/Sex predilection: Male preponderance, 3rd to 9th decades, most commonly 7th decade.
Risk factors if any: Not specified.
Associations: Retroperitoneal fibrosis, Sclerosing cholangitis, Riedel’s thyroiditis, Orbital pseudotumor.
Classification System:
Etymology and synonyms:
Mindelzun first described the regional change in mesenteric fat density on a CT as ‘misty mesentery’.
Synonyms are Lipodystrophy, Mesenteric panniculitis, Retractile panniculitis.
Treatment:
- If asymptomatic, no treatment is warranted.
- Medical treatment: Prednisone, colchicine, other immunosuppressants.
- Surgical treatment: Only if medical management fails, resection of mesenteric mass and adjacent bowel loops.
References:
Single best review article:
Other references:
- Buragina G, Magenta Biasina A, Carrafiello G. Clinical and radiological features of mesenteric panniculitis: a critical overview. Acta Biomed. 2019 Dec 23;90(4):411-422. doi: 10.23750/abm.v90i4.7696. PMID: 31910164; PMCID: PMC7233778.
- Filippone, A. et al. (2010) ‘Misty mesentery: A pictorial review of multidetector-row CT findings’, La radiologia medica, 116(3), pp. 351–365. doi:10.1007/s11547-010-0610-4.
Case co-authored by TeamGyan Member Dr. Bhargavi Sovani. Illustrations by Dr. Bhargavi Sovani.

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
Thank you. Nice case.
Glad you liked it, Michael. You can check out more cases here: https://radiogyan.com/radiology-cases