
TIRADS Introduction:
- With the advent of high-resolution ultrasound, the number of thyroid nodules being detected is increasing. Most of these nodules are benign. Even the smaller malignant nodules have an indolent course [1]. Also, the mortality associated with papillary thyroid carcinomas has remained low[1]. Hence it is essential to evaluate which of these nodules actually need a fine needle aspiration cytology (FNAC)/biopsy, which is the most effective method currently to diagnose whether a particular nodule is worrisome. Unnecessary biopsies can result in a burden on the healthcare system without significant benefits [1].
What is TIRADS / ti rads / TI-RADS and what does it stand for?
TI-RADS stands for Thyroid Imaging Reporting and Data System. It is a reporting system for thyroid nodules on Ultrasound formulated. It consists of guidelines regarding whether a thyroid nodule should be followed up on ultrasound or to should be biopsied.
What is TIRADS?
- Different variations of the TI-RADS classifications and recommendations are available, the most commonly followed one is the TI-RADS. A recent study published in AJR confirms that the TI-RADS performs well as compared to other scoring systems [2].
- Committee for TI-RADS has the following objectives [3]:
- Develop management guidelines for nodules that are discovered incidentally on CT, MRI, PET or ultrasound.
- Produce a lexicon to describe all thyroid nodules on sonography.
- Develop a standardized TI-RADS risk-stratification system based on the lexicon to inform practitioners about which nodules warrant a biopsy.
TIRADS Guidelines:
- The guidelines have been described as per the TI-RADS 2017 radiology white paper. The full text of this article is available here: TI-RADS white paper 2017 pdf.
- These guidelines provide criteria and recommendations for follow-up and biopsy of thyroid nodules.
- Similar to the BI-RADS classification, thyroid nodules on ultrasound are classified according to the risk of malignancies into the following categories [1]:
|
TIRADS classification |
||||
| Category | Points | Suspicion | Risk of Malignancy | Guideline |
| TR1 | 0 | Benign | 0.3% | No FNA |
| TR2 | 2 | Not suspicious | 1.5% | No FNA |
| TR3 | 3 | Mildly suspicious | 4.8 | If >2.5 cm: FNA
If >1.5 cm:Follow up at 1,3 ,5 years |
| TR4 | 4-6 | Moderately suspicious | 9.1 | If >1.5cm: FNA
If >1 cm:Follow up at 1,3 ,5 years |
| TR5 | 7 or more | Highly suspicious | 35 | If >1 cm: FNA
If >0.5 cm follow annually for 5 years |
FNA- Fine Needle Aspiration.
Download a ready to print image of the TIRADS classification
-
- One need not memorize this table, instead, you can print a copy of this TI RADS chart and put it up near your reporting station. Click here for a ready to print image of the table. Alternatively, you can use this image provided by the online [1]
- Thyroid nodules are evaluated on certain sonographic criteria, each criterion is allotted points which are summed up and then each nodule is categorized in one of the above-mentioned categories, depending on the score.
- Following criteria have been described:
TIRADS categories Spongiform* Mixed solid and cystic Solid or almost completely solid 0 1 2 Hyperechoic or isoechoic Hypoechoic Very hypoechoic 1 2 3 Taller-than-wide 3 Ill-defined: 0 points Lobulated/irregular Extrathyroidal extension 0 2 3 Large comet tail artefact# Macrocalcifications Peripheral/rim calcifications Punctate echogenic foci$ 0 1 2 3
Criteria
Categories
Points
Composition
Cystic or almost completely cystic
0
Echogenicity
Anechoic
0
Shape
Wider-than-tall
0
Margin
Smooth: 0 points
0
Echogenic foci
None
0
*Spongiform nodule should be composed predominantly (>50%) of cystic spaces.
# “Large comet-tail artifacts” are defined as echogenic foci with V-shaped echoes >1 mm deep to them.
$ Punctate echogenic foci are non-shadowing.
Download a ready to print image of the TIRADS categories
Note:
- Doppler has not found to be useful in distinguishing benign from malignant lesions, however, the presence of vascularity rules out debris and hemorrhage which are inconsequential [1].
- The presence of “halo” is not specific and is not included in the lexicon.
- Additional benign appearances are not included in the lexicon, for eg
- White knight: Uniformly hyperechoic nodule.
- Giraffe hide: Mixed hyper and hypoechoic areas.
- There is no mention of the role of thyroid elastography in the guidelines.
TIRADS Reporting guidelines for thyroid nodules:
- Nodules should be measured in three orthogonal planes.
- If there are multiple nodules, not more than 4 nodules should be documented.
- Definition of growth:
- More than 20% increase in at least two dimensions AND a minimal increase of 2mm OR
- More than 50% increase in volume.
- It is important to compare not just with the immediate previous studies, but with the previous ones as well.
- Number of nodules to biopsy: If multiple nodules are present, biopsy two nodules with the highest score, which may not necessarily be the largest nodules. Suspicious nodes if present should also be biopsied.
- Cervical nodes: Following suspicious features have been described [1]:
-
- Globular shape
- Loss of normal echogenic hilum
- Presence of peripheral rather than hilar flow
- Heterogeneity with cystic components
- Punctate echogenic foci that may represent microcalcifications.
-
A simplified approach to thyroid ultrasound and TI-RADS:
The interpretation guidelines in the White paper may seem complex to radiologists and sonologists.
- TIRADS atlas: TI-RADS Atlas with images for reference for each category.
- TI RADS Sonographer’s Worksheet
Thyroid Ultrasound Reporting Template using TIRADS:
Patient Identification:
Patient Demographics:
Indication:
Technique: Ultrasound examination of the thyroid and adjacent soft tissues was performed.
FINDINGS
Thyroid size:
Texture:
Estimated total number of nodules ≥1cm: 1, 2, 3, 4, 5, 6-10, >10]
Number of spongiform nodules ≥2cm not described below (TR1): [ ]
Number of mixed cystic and solid nodules ≥1.5cm not described below (TR2): [ ]
Nodule #: [1, 2, 3, 4]
Maximum size: [ ] cm; Other 2 dimensions [ ] cm Location: [right, left, isthmus];[upper, mid, lower]
Composition: [cystic/almost completely cystic (0), spongiform (0), mixed cystic and solid (1), solid/almost completely solid (2), cannot determine (2)]
Echogenicity: [anechoic (0), hyperechoic (1), isoechoic (1), hypoechoic (2), very hypoechoic (3), cannot determine (1)]
Shape: [not taller-than-wide (0), taller-than-wide (3)]
Margins: [smooth (0), ill-defined (0), lobulated/irregular (2), extra-thyroidal extension (3), cannot determine (0)]
Echogenic foci: [none (0), large comet-tail artifacts (0), macrocalcifications (1), peripheral calcifications (2), punctate echogenic foci (3)]
Additional echogenic foci 1:
Significant change in size (>/= 20% in two dimensions and minimal increase of 2 mm): [No/Yes]
Change in features: [No/Yes]
Change in TI-RADS risk category: [No/Yes]
TI-RADS total points: [ ] TI-RADS risk category: [TR1 (0 points), TR2 (2 points), TR3 (3 points), TR4 (4-6 points), TR5 (≥7 points)]
TI-RADS recommendation: [Ultrasound-guided fine needle aspiration, Follow-up ultrasound in 1 year, No further follow-up]
IMPRESSION:
TI-RADS recommendations
TR5 (≥7 points) – FNA if ≥ 1cm, follow-up if 0.5 – 0.9 cm every year for 5 years
TR4 (4-6 points) – FNA if ≥ 1.5cm, follow-up if 1 – 1.4 cm in 1, 2, 3 and 5 years
TR3 (3 points)- FNA if ≥ 2.5cm, follow-up if 1.5 – 2.4 cm in 1, 3 and 5 years
TR2 (2 points) & TR1 (0 points) – No FNA or follow-up
Alternatively, you can download the template from here: TI-RADS Diagnostic Ultrasound Reporting Template
TIRADS examples with scoring: Test yourself!
Go through the categories once again, use the TIRADS calculator and test yourself!
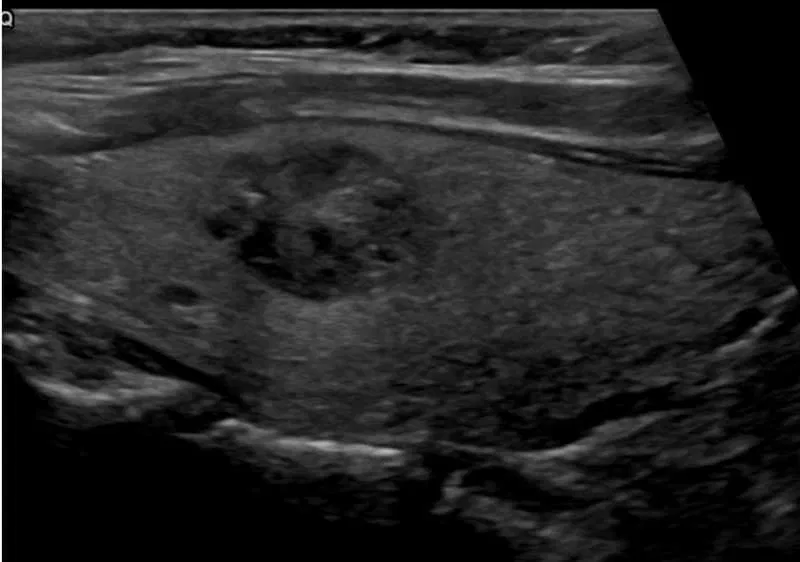
Example 1 :
What is the TIRADS score for this nodule?

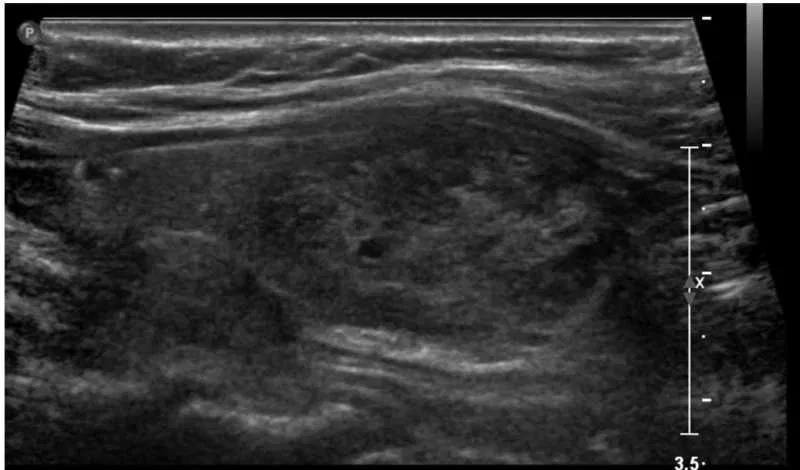
Example 2
What is the TIRADS score for this nodule?

Example 3:
What is the TIRADS score for this nodule?
Example 4:
What is the TIRADS score for this nodule?
If you got these wrong revise the guidelines here again.
Other useful TIRADS resources:
- TI-RADS Biopsy Reporting Template
- TI-RADS Atlas with images for reference for each category.
- TI-RADS Sonographer’s Worksheet
- TI-RADS guide for a description of features: TIRADS examples
- Thyroid Imaging Reporting and Data System (TI-RADS): A User’s Guide: A radiology article for reference.
References:
- Rumack Diagnostic Ultrasound
- Tessler FN, Middleton WD, Grant EG, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): white paper of the ACR TI-RADS Committee. J Am Coll Radiol 2017; 14:587–595.
- Middleton WD, Teefey SA, Reading CC, Langer JE, Beland MD, Szabunio MM, et al. Comparison of Performance Characteristics of American College of Radiology TI-RADS, Korean Society of Thyroid Radiology TIRADS, and American Thyroid Association Guidelines. AJR Am J Roentgenol. 2018;210(5):1148-54.
- TI-RADS. (2018). Acr.org. Retrieved 20 August 2018, from https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/TI-RADS
Visit the RadioGyan homepage for more radiology resources!

Improve Content And Help Your Colleagues!
Found an error in the post? Please let us know using our contact page and we will update it with due credits!
If you wish to contribute radiological images for this case (or any other article on the website), you can submit them here and you will be duly credited: Submit radiology case
Thank you
Welcome, Joha!